CHAPTER 5 Computed Tomography, Ultrasound, and Imaging-Guided Injections of the Hip
Computed tomography
Two- and Three-Dimensional Reformatted Computed Tomography Images
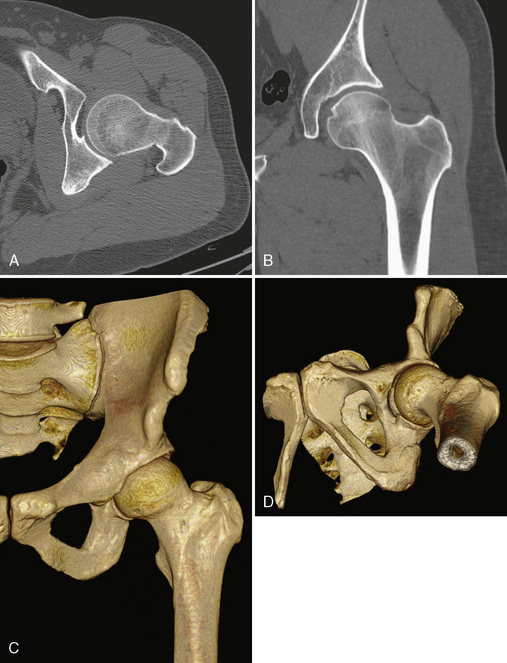
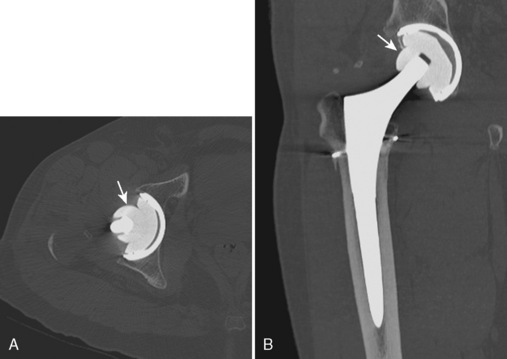
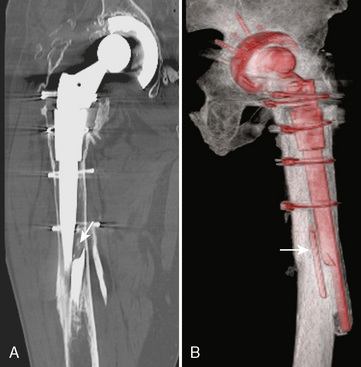
Before the invention of MDCT scanners, the ability to reformat the original axial data set into other imaging planes was markedly limited. The resulting images were often distorted with a venetian-blind effect with steplike contours, and thus they were of limited diagnostic quality. With the advent of MDCT scanners, however, this has dramatically improved. The reason behind this is the concept of isotropic imaging. If a volume of tissue (i.e., a voxel) is imaged at a very small quantity such that the length, width, and height of the volume are equal, then a reformatted image retains high resolution as compared with the axial images (Figure 5-1, A and B). It is possible to obtain these images with the use of MDCT scanners with 16 or more detector rows that allow for a slice thickness of less than 1 mm. A standard protocol for the imaging of any extremity with CT is to reconstruct the original data at a slice thickness of less than 1 mm with 50% overlap of each slice and to then produce two-dimensional reformatted images 1- to 2-mm thick in the axial, sagittal, and coronal planes. MDCT scanners now have several options or tools that allow for three-dimensional reformatted imaging and surface rendering. At an independent workstation, these data can be manipulated to remove overlying soft tissues, osseous structures, or hardware and to produce a rotating volumetric data set (Figure 5-1, C and D).
Femoroacetabular Impingement and Computed Tomography Arthrography
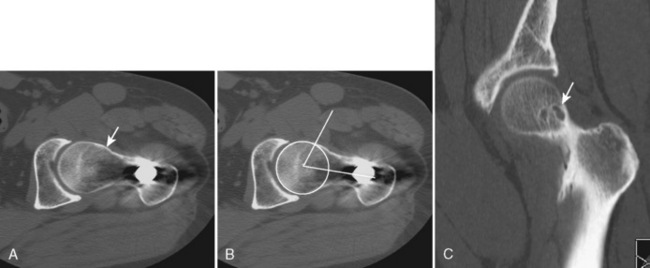
Many of the imaging features of FAI include bony abnormalities. Although magnetic resonance imaging (MRI) has also been used to demonstrate these findings, CT is well suited for characterizing bone abnormalities (Figure 5-2, A). With the cam type of FAI, the abnormal contour at the femoral head–neck junction is measured as the alpha angle, which indicates where the bone contour of the femoral head extends beyond the confines of the femoral head. An angle of more than 55 degrees measured on a sagittal–oblique image parallel to the femoral neck is considered abnormal and correlates with the cam type of FAI (Figure 5-2, B). Other bony changes associated with the cam type of FAI are well demonstrated with CT, including fibrocystic changes at the anterosuperior femoral neck (Figure 5-2, C). Such fibrocystic changes are more common among patients with FAI, and they may be directly caused by impingement. CT has an advantage over radiography for showing such cortical changes. Other radiographic signs of the cam type of FAI, such as the abnormal contour of the femoral head–neck junction (pistol grip deformity), are also well delineated on CT, because patient positioning may not optimally profile the bone contour deformity.
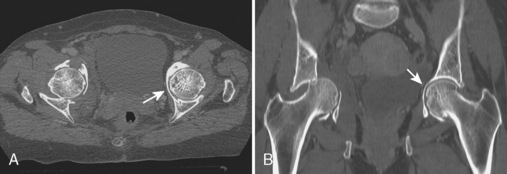
With regard to CT of the pincer type of FAI, bony abnormalities such as acetabular protrusion (Figure 5-3) and acetabular retroversion may be demonstrated. When assessing for acetabular retroversion on radiography, the crossover sign (i.e., the anterior acetabular wall projects lateral to the posterior acetabular wall) may be affected by patient positioning. CT avoids this pitfall by directly measuring the acetabular version, which is described as 23 degrees in females (range, 10 to 37 degrees) and 17 degrees in males (range, 4 to 30 degrees). A retroverted acetabulum is associated with the pincer type of FAI and with hip osteoarthrosis. CT is also effective for measuring anterior and posterior acetabular sector angles in the setting of hip dysplasia.
Hip Trauma
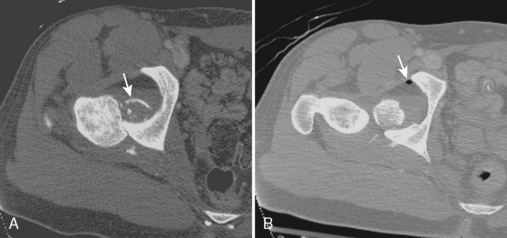
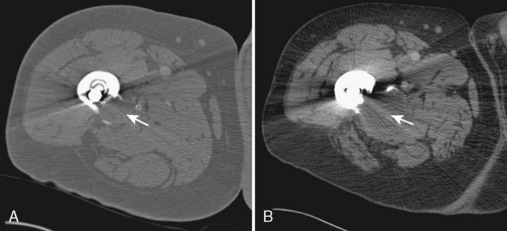
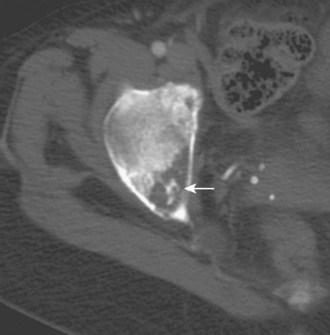
CT is often used to evaluate the hip and acetabulum after hip dislocation and other pelvic trauma (Figures 5-3 and 5-4). When an acetabular fracture is identified by radiography, CT can further characterize the fracture pattern with the use of multiplanar reformatted images and three-dimensional surface rendering (see Figure 5-3). Associated abnormalities such as intra-articular bodies and pelvic hematoma are also well demonstrated with CT. After hip dislocation, CT demonstrates the position of the femoral head and the coexisting femoral head fracture (see Figure 5-4, A). A sign of prior hip dislocation on CT is the presence of a bubble of gas, which is most commonly seen at the anterior aspect of the hip joint (see Figure 5-4, B).
It is important to understand the advantages and disadvantages of CT for the evaluation of fracture. CT is most accurate for demonstrating fractures of cortical bone (Figure 5-5, A). In an osteopenic patient in whom the cortex is thin, accuracy will decrease, especially when the fracture is not displaced. This becomes even more problematic for the diagnosis of an intramedullary fracture. In an osteopenic patient in whom the trabeculae are thin or resorbed, a fracture may not be apparent on CT. MRI has been shown to be more accurate than CT for the evaluation of proximal femur fractures in patients more than 50 years old where CT led to a misdiagnosis in 66% of patients. In addition, CT may not show the entire intramedullary extent of a presumed isolated greater trochanteric fracture. As a general rule, CT is most effective for diagnosing fractures of cortical bone in younger patients, and it is relatively limited with regard to intramedullary fractures among the elderly (e.g., insufficiency-type stress fractures). By contrast, a chronic-fatigue–type stress fracture is well demonstrated with CT given the associated sclerosis (Figure 5-5, B).

Hip Arthroplasty
Although radiography is the imaging method of choice for the routine evaluation of the hip after arthroplasty, CT does have a role in specific scenarios, such as the evaluation of infection, osteolysis, and component position. The technical advance that permits for the CT evaluation of metal with reduced artifact is MDCT, which allows increased x-ray tube current to image through metal. The individual components of an arthroplasty as well as the adjacent soft tissues and bone can be visualized with CT (Figure 5-6). This is helpful for displaying fracture (Figure 5-7) and for the diagnosis of soft-tissue infection adjacent to a prosthesis (Figure 5-8). In the presence of component wear and particle disease, CT can directly show the polyethylene component wear as well as the adjacent osteolysis (Figure 5-9). Although radiography adequately screens for osteolysis, CT more accurately measures the volume of osteolysis. CT can also be used to measure component version after hip arthroplasty.
Miscellaneous Hip Abnormalities
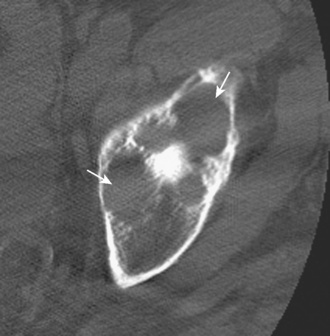
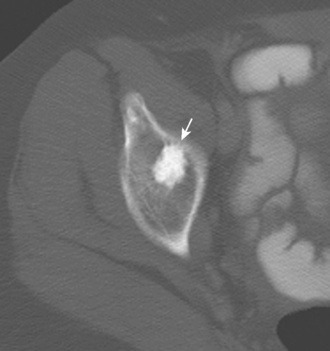
Other hip disorders that involve the bone or that produce calcification or ossification can be evaluated with CT. Primary synovial osteochondromatosis is a benign neoplastic condition in which hyaline cartilage nodules form in the subsynovial tissue of a single large joint. If these nodules ossify, they are readily demonstrated on CT as multiple uniform ossific bodies in the joint (Figure 5-10). Secondary osteoarthrosis and associated erosions may also be present. The hip is the second most common joint affected by this condition, after the knee.
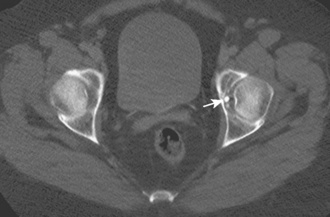
Figure 5–10 Synovial osteochondromatosis. Axial CT image shows several ossified cartilaginous bodies (arrow).
Osteoid osteoma is a benign bone lesion of uncertain origin that involves a vascularized nidus being present within the bone, typically the cortex. When this occurs in an extra-articular location, the nidus is associated with significant sclerosis and periostitis (Figure 5-11). When it is intra-articular, there is associated effusion and synovitis. CT shows the nidus as a round area of low attenuation with surrounding sclerosis that may calcify. CT can be used to effectively guide the percutaneous thermoablation of osteoid osteomas.

CT may also be used to characterize other bone abnormalities. When a sclerotic focus is present within the bone, CT can show the uniform sclerotic density and spiculated margins that are typical of a bone island or enostosis (Figure 5-12). The calcified matrix of a chondroid tumor such as chondroblastoma or chondrosarcoma (Figure 5-13) or the ossified matrix of an osteosarcoma can be demonstrated with CT, which assists with the characterization of a primary bone tumor. CT is the typical imaging method used for the percutaneous imaging-guided biopsy of a bone tumor that involves the pelvis or the proximal femur.
Ultrasound
< div class='tao-gold-member'>
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


