CHAPTER 19 Arthroscopic Femoral Osteoplasty
Introduction
In 1995, Ganz first described femoroacetabular impingement (FAI), and, in 1999, it was introduced into the English literature. Although the first case was pincer impingement as a result of acetabular overcoverage after a periacetabular osteotomy, further investigations by Professor Ganz and his group led to the recognition of a second type of impingement: cam impingement. This type of impingement is the result of loss of the femoral head–neck offset, which causes the joint to function like a mechanical cam device. The anatomy of cam impingement has been previously described as a pistol grip deformity or a tilt deformity (Figure 19-1). Many investigators have attributed this anatomy to subclinical slipped capital femoral epiphysis (SCFE), and certainly the residuals of an unreduced SCFE can result in cam impingement. Beaule and colleagues demonstrated in a computed-tomography–based study that cam impingement can occur without SCFE, which suggests that this condition is not the result of a subclinical SCFE. Wagner and colleagues demonstrated that the bone of the cam lesion is not reactive nor does it involve any inflammation; thus it is not likely the result of the impingement or arthritis. Because the deformity occurs at or near the femoral head physeal scar, it may be genetically predetermined or the result of stresses applied during development. Either way, this pistol grip deformity has been associated with premature osteoarthritis of the hip. It has also been suggested that cam impingement results in premature or idiopathic arthritis of the hip. However, Bardakos and Villar have shown that only two thirds of patients with cam impingement show radiographic progression of arthritis at 10-year follow up.
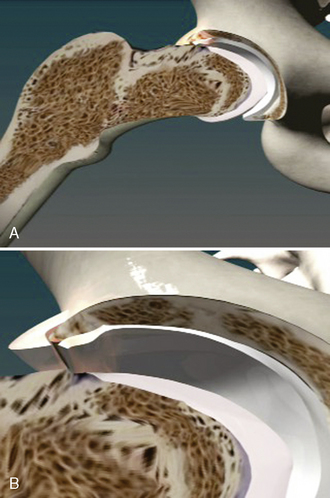
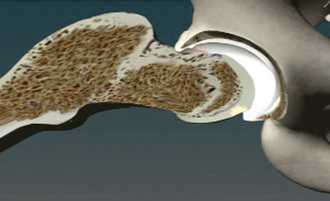
The anatomy of cam impingement can frequently be seen among those patients with idiopathic arthritis, although this is still a controversial subject. The suggestion that impingement results in hip arthritis is also likely when studying the pathologic findings of symptomatic impingement patients without arthritis, particularly of those with labral tears and chondral lesions that are thought to progress to arthritis when untreated. The majority of patients in Ganz’s series had a combination of cam and pincer impingement, which has been confirmed in other published series as well as my own experience of several hundred patients with symptomatic FAI. Beck and colleagues found that the demographics and pathology do correlate with the different subtypes of impingements. Particularly, for those with isolated types of impingements, the cam type is the most common (17%). It tends to occur in 19-year-old males, whereas those with isolated pincer impingement are 40-year-old active females. For those with isolated cam impingement, the common pathologic findings initially are focal, deep chondral delamination lesions (anterolaterally and extending about 1 cm from the acetabular edge) (Figure 19-2). At first the labrum is intact, but it eventually separates from the acetabular articular cartilage edge before degenerating. The labrum often separates from the acetabulum and the articular cartilage, and the articular cartilage delaminates from the bony acetabulum (Figure 19-3). Alternatively, those with pincer impingement tend to have intrasubstance crushing of the labrum, and the articular cartilage damage extends only a couple of millimeters from the acetabular edge (Figure 19-4). Although the greatest depth of penetration of articular cartilage damage in pincer impingement is also anterolateral, the damage tends to be more global and to extend around the circumference of the acetabulum. In addition, there is often posterior acetabular (62%) and femoral head (31%) articular cartilage damage as a result of the contrecoup phenomenon of the femoral head levering against the anterior acetabulum as the patient tries to obtain hip motion, which results in shearing forces posteriorly (see Figure 19-4). It has been my experience that one type of impingement will predominate the intra-articular pathologic findings.
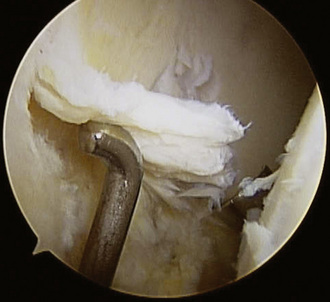
Figure 19–2 Arthroscopic view of the chondral delamination of the acetabulum associated with cam impingement.
Indications
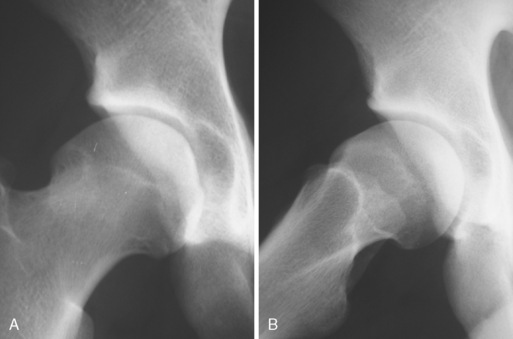
Although some believe that FAI results in arthritis and thus that surgery should be performed to prevent the arthritis, that has not been the approach used in our practice, because there is no evidence at this point that arthritis can be prevented. I certainly believe that having the anatomy of impingement does put the patient at risk for chondral injury, labral injury, and, potentially, arthritis. However, on the basis of my experience with patients who are more than 60 to 70 years old with the anatomy of FAI but no evidence of arthritis or hip symptoms in combination with my extensive experience of cadaveric research involving specimens 80 to 90 years old with the anatomy of obvious cam and combined impingement without evidence of arthritis, I have concluded that not everyone with the anatomy of FAI will develop osteoarthritis (Figure 19-5). It is my belief that the anatomy of FAI does put patients at potential risk for joint damage. However, it likely requires the individual to be involved in activities that require greater hip range of motion with or without pivoting (e.g., martial arts, soccer, running, golf) to result in impingement. After the tissues start breaking down, patients develop symptoms, because the labrum is a structure that is richly innervated. It is as soon as patients have confirmed intra-articular pain that surgery is indicated. Intra-articular anesthetic guided by fluoroscopy or ultrasound and that is given by itself or with contrast when performing magnetic resonance arthrography is a useful diagnostic test to confirm that the joint is the source of pain. Thus, the goal of surgery is to relieve intra-articular hip pain that is the result of impingement.

Thus, indications for surgery include the following:
History and physical examination
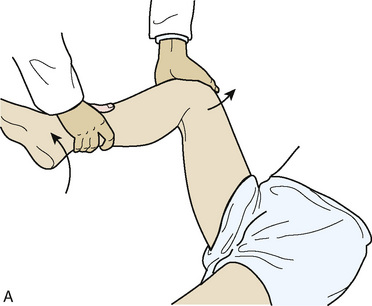
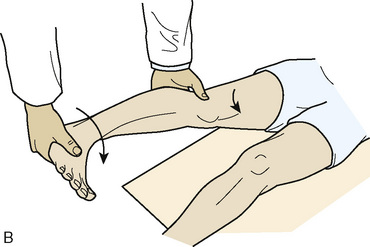
Although a complete discussion of the evaluation of the hip is beyond the scope of this chapter, a brief discussion of the general concepts is appropriate. First, evaluation includes the inspection of the gait and of the skin around the hip. Patients are assessed for hip weakness and tightness with the use of the Trendelenburg and Ober tests. Hip range of motion is assessed while the patient is supine. Evaluation of hip adduction and abduction, as well as internal and external rotation, should be performed in hip flexion and extension. Also, hip motions evaluated include flexion, extension, and flexion contracture. There is usually limited hip internal rotation, particularly when the hip is in flexion, among patients with impingement. Furthermore, patients frequently have pain when the hip is flexed to 90 degrees, adducted, and internally rotated; this is known as the impingement test (Figure 19-6). The labral stress test and the resisted straight-leg raise are tests that commonly result in hip pain among patients with labral tears and symptomatic impingement (Figure 19-7). These tests are often positive among patients with both cam and pincer types of FAI, and they may also be positive among patients with other sources of intra-articular hip pain.

Imaging and diagnostic tests
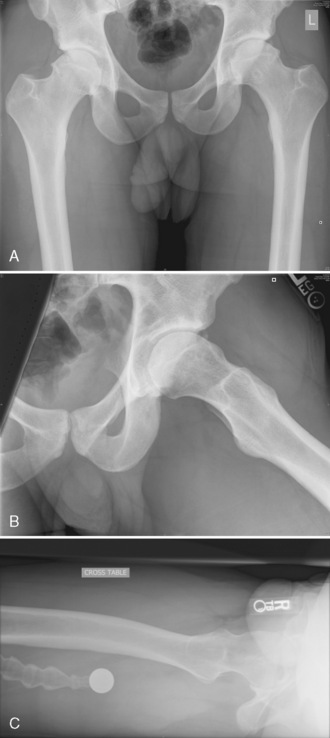
Plain radiographs are extremely valuable for the assessment of patients with hip pain that is the result of hip impingement. The standard imaging series for patients with hip pain includes an anteroposterior pelvic view with the coccyx centered 1 cm to 3 cm above the pubic symphysis and a true cross-table lateral radiograph (Figure 19-8). A frog-leg lateral view will demonstrate a lateral projection of the proximal femur and thus can be used for cam impingement assessment; however, this is not a lateral view of the acetabulum, so it has limited usefulness (see Figure 19-8, B). A cross-table lateral view, a Dunn view, and a modified Dunn view are true lateral views of the hip that can provide more information about the acetabulum (see Figure 19-8, C). The femoral head is generally symmetric, particularly the head–neck offset. A loss of the sphericity of the femoral head–neck region may be consistent with cam impingement (see Figure 19-8, A through C). This can be seen as a flattening of the concave surface of the lateral femoral neck and the appearance that the femoral head is not centered over the femoral neck. Leunig and colleagues demonstrated that, for patients with hip dysplasia, the apex of the femoral head is approximately 1 cm beyond the low point of the femoral neck, whereas in patients with impingement this distance was only 3 mm. In some situations, there may be a bump on the anterolateral surface of the femoral neck that may project beyond the femoral head or have a sharp transition or even a hook appearance at the head–neck junction. The alpha angle was originally described by Notzli and colleagues to quantify the head–neck offset on radially generated axial magnetic resonance imaging cuts of the femoral neck and head. These authors demonstrated that, in their normal population, the alpha angle averaged 42 degrees, whereas in those patients with impingement, this angle averaged 74 degrees. Most surgeons use 50 degrees or 55 degrees as their cutoff point for defining cam impingement. This angle has also been used when evaluating plain radiographs and computed tomography scans, although it has not been validated for these modalities. Additional plain radiographs may demonstrate a short femoral neck or a femoral neck–shaft angle that is varus, which may result in cam-type impingement. Untreated or residual deformity from SCFE or Legg-Calvé-Perthes disease may be seen on plain films, and this may result in cam impingement. Pincer impingement may also be seen on plain radiographs in association with coxa profunda, protrusio, retroversion, or relative retroversion of the superior acetabulum and arthritic changes.
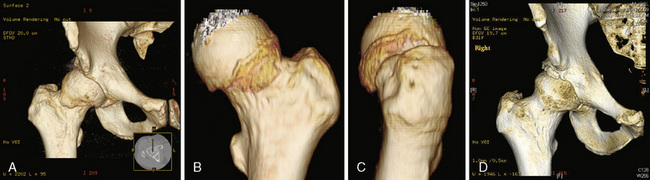
Computed tomography scans, particularly three-dimensional ones, are particularly useful for demonstrating the bony anatomy associated with cam impingement (Figure 19-9). Magnetic resonance imaging, particularly magnetic resonance arthrography, is beneficial for demonstrating the cam lesion by allowing for a way to measure the alpha angle and to demonstrate labral tears, edema, or cysts within the femoral neck (these are often seen with impingement); this type of imaging can occasionally demonstrate chondral lesions (Figure 19-10). Local anesthetic is usually introduced with the contrast used for magnetic resonance arthrography to determine whether the pain is temporarily relieved within the joint, which confirms the source of pain as being intra-articular.
< div class='tao-gold-member'>
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


