The adoption of arthroscopic techniques has led to an overall decrease in many complications associated with knee surgery. Arthroscopic meniscectomies, in fact, have become so routine that both patients and surgeons often view it as nearly risk free. Multiple series have been published over the years showing that this view is overly optimistic. The results of a survey performed by the Arthroscopy Association of North America (AANA) were published in 1985 and reported an overall complication rate of 0.3% (1). In 1986, Sherman et al (2). reported an 8.2% complication rate in a retrospective review of 2,640 patients, having routine arthroscopic knee procedures not involving ligament reconstruction. Small published several reports culminating in the 1988 review of a registry of cases performed by 21 experienced arthroscopists over a 19-month period compiled by the Complications Committee of AANA. The complication rate for knee arthroscopy was 1.8% (3). More recently, Reigstad and Grimsgaard (4) reported a 5% complication rate in 876 simple knee arthroscopies performed between 1999 and 2001. The rate of complications requiring intervention was 0.68%. When the full range of arthroscopic procedures in the knee is taken into consideration, the rate of complications is significantly higher. The goal of this chapter is to give an overview of the most significant and most common complications associated with common arthroscopic procedures of the knee and to offer guidance on the prevention, identification, and treatment of those complications.
INFECTION
Postoperative infection after knee arthroscopy is fortunately quite rare. Deep infection rates have been reported as being less than 0.3% (1, 2, 3 and 4). Superficial wound healing problems are somewhat more common. The infection rate for ACL reconstruction, however, has been reported to be as high as 1.74%, with a mean incidence in the literature of 0.52% (5, 6). Most infections are felt to be due to inoculation at the time of surgery, but concomitant infection at the tibial tunnel site is common, suggesting communication to the joint from an infected superficial wound was possible (7, 8). Rapid diagnosis and treatment of intra-articular infection is important, as the loss of glycosaminoglycan in cartilage begins within 8 hours and can progress to cartilage loss and degenerative changes, full-thickness cartilage defects, and osteomyelitis (5, 8, 9, 10 and 11). With prompt treatment, postoperative infections can be eradicated.
Most patients with postoperative knee infections present in the acute (<2 weeks) or subacute (<2 months) periods (12). It has been noted that presenting symptoms of postoperative infection can be confused with postoperative changes. In fact, Schollin-Borg et al. (5) reported that 60% of the time there was a failure to appreciate an infection at the first visit. The classic presentation is an acutely swollen painful knee with limited range of motion (12). Increased pulsatile pain, painful range of motion, rapidly increased and persistent effusion, incision drainage, local erythema, and warmth with intermittent fever are common symptoms as well. A subtle increase in pain and difficulty in physical therapy should be seen as ominous signs (8, 13). If there is clinical suspicion of a joint infection, the knee should be aspirated and the fluid sent for cell count, Gram stain, and cultures. Fluid analysis for glucose, protein, and LDH may be helpful as well. The sensitivity and specificity of each test is shown in Table 83.1. Given the relatively low specificities of most tests, the data should be viewed as a whole. The most common organism found in culture is Staphylococcus aureus, which is present in 48.5% of positive cultures. The second most common is Staphylococcus epidermidis, which is present in 39.5% of positive cultures. Gram-negative bacteria were present in 7% of cases and anaerobes in 11.5% cases (6). Infection after allograft reconstruction should raise concern for allograft contamination, particularly when the cultured organisms are atypical (15).
The primary goal in treating an infection after ligament reconstruction is protection of the articular surface (16). Arthroscopic debridement with extensive synovectomy using accessory portals has been shown to decrease the bacterial load in the joint (7). Although some authors have advocated graft removal and early reimplantation, most surgeons prefer to save the graft if possible (13, 17). In their systematic review, Mouzopoulos et al. (12) suggested a protocol for treatment after ligament reconstruction. The graft should be removed only if it is unstable, if it is impregnated by thick purulent exudates, or if cultures have shown S. aureus and antibiotic treatment was significantly delayed. Empirical IV antibiotic therapy should be broad. A thorough arthroscopic synovectomy should be carried out using 10 to 15 L of fluid and accessory wounds should be opened if they are at all suspicious. If there is any exudate on the graft, it should be removed. They recommend leaving wounds open and using continuous irrigation drains if felt necessary. Repeat arthroscopy should be performed every 2 to 3 days as needed. Parenteral antibiotic therapy should be narrowed per culture results and continued for 6 weeks. Oral antibiotics should follow for another month. With careful treatment, the graft can be retained and the patient can expect a good outcome (18).
Table 83.1 Laboratory analysis of serum and joint aspirate sensitivities and specificities for joint infection (14)
Laboratory Analysis
Laboratory Value
Sensitivity (%)
Specificity (%)
Joint aspirate
WBC > 100,000/μL
29
99
Joint aspirate
WBC > 50,000/μL
62
92
Joint aspirate
WBC > 25,000/μL
77
73
Joint aspirate
Polymorphonuclear cells ≥ 90%
73
79
Joint aspirate
Synovial fluid glucose < 1.5 mmol/mL
51
85
Joint aspirate
Protein > 3.0 g/dL
48
46
Joint aspirate
LDH > 250 U/L
100
51
Serum lab values
WBC > 10,000/μL
90
36
Serum lab values
Erythrocyte sedimentation rate > 30 mm/h
95
29
Serum lab values
C-reactive protein
77
53
Intraoperative Graft Contamination
Studies have shown culture evidence of autograft contamination in 13% of uncomplicated ACL reconstructions despite no clinical evidence of postoperative infection (19, 20). Although rare, intraoperative graft contamination due to a break in sterile technique is possible. Izquierdo et al. (21) surveyed sports medicine specialists and found that 25% of 196 respondents had experienced a total of 57 intraoperative graft contaminations. In 75% of those cases, the graft was cleansed and implanted. There were no reported postoperative infections. The most common cleansing technique was soaking the graft in Chlorhexidine solution, and the paper concluded that this represented the standard of care. The efficacy of Chlorhexidine soaks has been supported by basic science papers as well (22, 23). In reporting his experience with three contaminated ACL grafts, Pasque notes that the risk appears to be higher when there is turnover in the surgical team. He noted no postoperative infections after rinsing the grafts in Chlorhexidine followed by a triple antibiotic bath (24). Authors have noted that Chlorhexidine is potentially chondrotoxic, so a subsequent antibiotic soak serves the dual purpose of completion of graft sterilization and as a rinse. The use of antibiotic soaks alone, however, is not recommended (25).
ARTHROFIBROSIS
Localized Arthrofibrosis
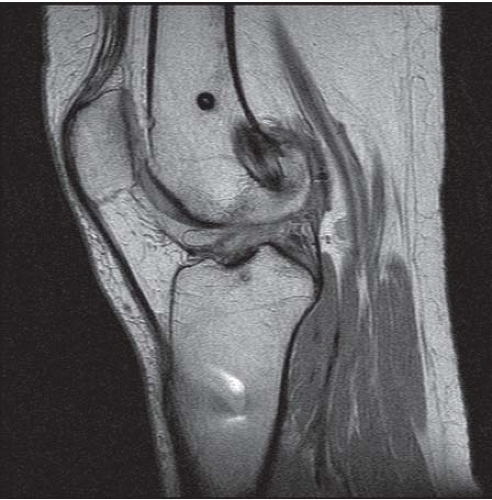
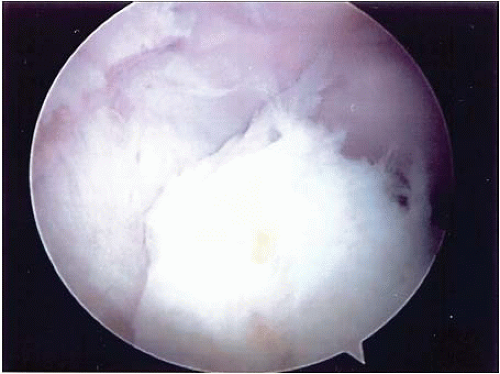
Infrapatellar contracture syndrome is a pathologic fibrous hyperplasia of the infrapatellar fat pad. It has been described as having three stages beginning with periarticular inflammation, edema, and quadriceps weakness. After 6 weeks, this progresses to limited patellar mobility, inferior patellar tilt, and a flexed knee gait. After 8 months, patellar mobility improves, but the patella baja remains and patellofemoral degenerative changes begin (26, 27). Scarring in the anterior interval leads to tethering of the patellar tendon, pain, and loss of extension (28). The fat pad itself appears to be important in the pathogenesis, and the syndrome has been associated with acute surgery, patellar tendon autograft, and multiple surgical procedures (27). Prevention consists of minimizing injury to the fat pad at the time of procedure and starting aggressive rehabilitation in the early postoperative period. Treatment should focus on allowing the inflammation to decrease by backing off on physical therapy, performing passive patellar mobilization. Nonsteroidal anti-inflammatory drugs (NSAIDs) and oral corticosteroids may be useful as well. In chronic cases, a low signal area of scar coursing from the fat pad to the anterior tibia can be seen on MRI (Fig. 83.1). Patients often have a positive Hoffa test, defined as pain in the anterior knee with pressure near the patellar tendon with knee extension. Good results have been seen with arthroscopic debridement using a high-viewing portal (Fig. 83.2) (28).
FIGURE 83.1. Scar tissue interposed between fat pad and tibia.
Generalized Arthrofibrosis
There appears to be a genetic predisposition to excessive scarring after trauma or surgery. Skutek et al. (29) have reported that certain HLA types are at increased risk. Studies have shown that the fat pad is capable of releasing proinflammatory cytokines, which may contribute to the inflammatory response in the joint (27, 30, 31 and 32). Given this association with fat pad injury, authors have suggested that minimizing trauma to the fat pad at the time of surgery may help limit the risk or generalized arthrofibrosis (26, 33).
FIGURE 83.2. Arthroscopic view of anterior compartment scar tissue.
There is a clear association between multiple ligament injuries and arthrofibrosis. Injury to the MCL and ACL together is a particular problem. Bracing the MCL and allowing it to heal before reconstructing the ACL may minimize the risk. In cases of grade 3 MCL injury, a tear above the joint line increased arthrofibrosis risk (34). In repairing the MCL, surgeons must take care not to tie the MCL down too close to the joint line.
In addition to taking meticulous care at the time of surgery to minimize trauma to the joint, injury to the fat pad, and postoperative hemarthrosis, surgeons can limit the risk of arthrofibrosis by encouraging aggressive rehabilitation. Special attention should be paid to regaining full extension early. Some authors have recommended the use of bracing to help with extension, but a recent systematic review of bracing found no benefit (35). There is evidence that acute ACL reconstructions are associated with increased risk of arthrofibrosis. The consensus appears to be that surgery should be delayed until the knee has become less swollen and inflamed and full extension is restored (33, 36, 37 and 38).
Early treatment for motion loss consists of carefully managed rehabilitation. If there is evidence of significant joint inflammation, it is important not to push the knee too hard to allow it to settle down. If no inflammation is appreciated, an aggressive phased physical therapy program is warranted, focusing on full knee extension. Authors have differed on the usefulness of manipulation under anesthesia (35, 39, 40 and 41). There appears to be agreement that manipulation is best in cases of mild arthrofibrosis with problems in flexion. If conservative treatments fail, aggressive arthroscopic treatment has been advocated (Fig. 83.3). Millett and colleagues (35) have outlined a nine-point arthroscopic release that ensures careful assessment of all areas in the joint that could contribute to the problem. If arthroscopic treatment fails, an aggressive open surgical salvage treatment that has offered good results (42).
FIGURE 83.3. Arthroscopic view of adhesions in the suprapatellar pouch.
DEEP VENOUS THROMBOSIS AND VENOUS THROMBOEMBOLISM
The incidence of deep venous thrombosis (DVT) after arthroscopic surgery has been reported to be as low as 0.6% when purely clinical diagnostic criteria are used and as high as 41% diagnosed using MR venogram (43, 44). Most clots after knee arthroscopy appear to be below the knee, and reports of fatal PE after knee arthroscopy are rare (45, 46, 47, 48 and 49). Two papers specifically looking for surgical and patient factors associated with increased DVT risk showed that tourniquet time longer than 60 minutes and prior history of DVT are the only significant factors (50, 51).
In their Cochrane Database Review, Ramos et al. (49) found that treatment with low molecular weight heparin offered a relative risk of 0.16 for DVT when compared with control. This was balanced by a relative risk of 2.04 for minor complications such as hemarthrosis and gastric bleeding. The only patient with a PE in their pooled data was in the treatment group. They concluded that “no strong evidence was found to conclude thromboprophylaxis is effective in preventing thromboembolic events.”
The American College of Chest Physicians released their recommendations on thromboprophylaxis after the Eighth ACCP Conference on Antithrombotic and Thrombolytic Therapy in 2008. After their review of the literature, they concluded that the risk of VTE appears to be low in arthroscopic procedures when compared with major orthopedic procedures. They note that the results of three studies have shown a decrease in the rate of asymptomatic DVT through LMWH use, but that adverse bleeding events were increased. They felt that patients should be encouraged to mobilize as soon as possible after surgery. The formal recommendations were that no routine thromboprophylaxis other than early mobilization be used in patients with no thromboembolic risk factors. They did, however, recommend LMWH thromboprophylaxis of an unspecified duration if the patient has any of the risk factors in Table 83.2 or if the procedure is unusually long or complicated (52).
VASCULAR COMPLICATIONS
Vascular injury associated with arthroscopy is rare. In two reports by Small (3, 53), there were no vascular injuries in 9,791 knee arthroscopies. Sherman et al. (2) reported no vascular complications in 2,640 cases. DeLee (1), however, reported nine cases of penetrating artery injuries in 118,590 arthroscopies. Six were popliteal artery injuries, resulting in four amputations. Popliteal artery injuries are typically associated with PCL reconstruction and repairs of the posterior horn of the meniscus (54, 55). There are two reports, however, of popliteal injury associated with ACL reconstruction (56, 57). With the knee in flexion, the popliteal artery lies an average of 29.13 mm posterior to the PCL at its midpoint, and only 9.69 mm from its tibial insertion (58). The artery has been shown to be farther from the PCL in 100° of knee flexion than it is in lesser angles (59). It has also been noted that with the leg in external rotation the artery is brought into proximity to the posterior horn of the lateral meniscus (60). Penetrating injury to the popliteal artery can cause a pseudoaneurysm. About 30% of these are asymptomatic. Symptoms generally become apparent 2 to 3 weeks after surgery and can include a popliteal mass, claudication, venous stasis, neurologic changes, ischemia, and thrombotic events. The amputation rate has been reported to be over 20%. Vascular imaging and rapid referral to a vascular surgeon are essential (57, 61).
Table 83.2 Risk factors for VTE Geerts et al. (52)
Surgery
Trauma (major trauma or lower extremity injury)
Immobility, lower extremity paresis
Cancer (active or occult)
Cancer therapy (hormonal, chemotherapy, angiogenesis inhibitors, radiotherapy)
Estrogen containing oral contraceptives or hormone replacement therapy
Selective estrogen receptor modulators
Erythropoiesis-stimulating agents
Acute medical illness
Inflammatory bowel disease
Nephrotic syndrome
Myeloproliferative disorders
Paroxysmal nocturnal hemoglobinuria Obesity
Central venous catheterization
Inherited or acquired thrombophilia
Given the proximity of the popliteal artery to the PCL, care must be exercised in PCL reconstructions. Guides that capture the pin as it exits the posterior tibia are advisable to avoid overpenetration (55). Surgeons would be wise to perform their posterior notch work for both PCL and ACL reconstruction with the knee at a high flexion angle to minimize risk to posterior structures. Care must be taken in creating posterior portals, as there is risk to the popliteal artery from both the spinal needle and the cannula (62). Injury to the popliteal artery has been described after both medial and lateral posterior horn meniscectomies (60, 63).
Use of bicortical screw fixation like a post and washer for ACL graft fixation puts the popliteal artery at risk below the joint line (56). This risk is minimized by aiming toward the fibula when drilling through the posterior tibial cortex. With appropriate trajectory, the popliteal artery and vein were on average 11.4 mm from the drill hole, although in one specimen, the distance was only 3.5 mm (64).
The popliteal artery is also at risk during meniscal repair. When an inside-out technique is used, retractors should be placed to capture the needles and they should be passed under direct visualization (65). Needles should be directed away from the posterior midline. With all inside meniscal repair systems, the surgeon must be careful to avoid overpenetration as well, particularly in the posterior horn of the lateral meniscus, which is closest to the popliteal artery (66). Depth limiters should be used, as studies have shown that some devices can come within 3 mm of the artery (67).
Injury to the medial inferior geniculate artery has been associated with hamstring tendon harvest and medial periosteal stripping in the area of the tibial tunnel entrance (68, 69). The medial and lateral inferior geniculate, descending geniculate, and sural arteries have all been injured during meniscectomies as well (68, 70, 71 and 72). Recognition of these injuries, which can cause heavy bleeding and hematoma, may allow ligation of the artery. Saphenous vein injury has been reported with all-inside meniscal repair techniques causing persistent hematoma (73).
NEUROLOGIC COMPLICATIONS
Neurologic complications after knee arthroscopy are rare. Large reviews have placed the incidence at between 0.01% and 0.6% (1, 3, 53, 74, 75). Lesions of the common peroneal nerve have been reported after routine knee arthroscopy through both traction and direct injury during lateral meniscectomy (76, 77). Peroneal injuries are most commonly associated with needle injury or suture entrapment during lateral meniscal repair (53, 78, 79, 80 and 81). When performing an inside-out meniscal repair, a posterolateral incision made at the joint line behind the lateral collateral ligament should be used. With the knee flexed 90°, dissection is carried between the biceps femoris tendon and the iliotibial band to allow placement of a retractor under the lateral head of the gastrocnemius on the posterolateral joint capsule. The needles can be retrieved and tied under direct visualization (82). If the nerve function is decreased after a repair, release of the sutures has been reported to result in complete recovery (81, 83). Two studies have shown that the peroneal nerve is at a small risk of injury when drilling the posterolateral femoral tunnel during double-bundle ACL reconstruction. Higher knee flexion angles of 110° to 120° minimize that risk (84, 85).
The neurologic structures most at risk with ACL reconstruction are the superior and inferior trunks of the infrapatellar branch of the saphenous nerve (86). Laceration of the nerves causes numbness and dysesthesia lateral and distal to the incision and can lead to painful neuromas (87). This can lead to bothersome anterior knee pain and possible complex regional pain syndrome (CRPS). The nerve is at risk at the time of skin incision from hamstring and patellar tendon harvest, tendon stripping, and drilling of the tibial tunnel. Risk of injury during patellar tendon harvest can be lowered by using horizontal incisions or two spaced vertical incisions (88, 89). A traditional longitudinal incision is less likely to injure the braches if it is made with the knee in full flexion as this moves the branches distally (86). If the branches can be identified at the time of surgery, an effort should be made to protect them. Injury can occur during hamstring harvest as well (90). The nerve lies just superficial to the gracilis tendon. With a traditional vertical incision for hamstring harvest, 68% of patients have been shown to have sensory disturbances affecting an average surface area of 48 cm2. By making an oblique incision that follows the path of the tendons, only 24% of patients have sensory disturbance over a much smaller 8.4 cm2 (91). It has been suggested that the tendons should be harvested with the knee flexed and hip externally rotated in order to minimize tension on the nerve during harvesting (92). Management of symptomatic injury to the infrapatellar branch includes padding, physical therapy, and direct skin desensitization. It is important to continue aggressive mobilization to minimize risk of CRPS.
The saphenous nerve is also at risk during inside-out meniscal repair. A retractor should be placed on the posterior capsule through an incision made just above the joint line behind the medial collateral ligament. With the knee at 90° of flexion to keep the infrapatellar branch 1 cm proximal to the joint line, the sartorius fascia is opened and the interval between the fascia and the capsule can be exploited. Care should be taken to avoid the sartorial branch of the saphenous nerve, as it can often be encountered in this incision (93). Transillumination may help identify the location of the saphenous vein that runs with the nerve (94). Needles in inside-out repairs can be passed under direct visualization (82, 87).
The tibial nerve is at small risk in repair of the posterior horns of both the medial and the lateral menisci. Placement of retractors as described and directly insideout needles away from the center of the popliteal fossa should minimize the risk. Because the tibial nerve lies in proximity to the popliteal artery behind the knee, techniques described to minimize vascular complications during PCL reconstruction should also protect the tibial nerve.
Modern suture-based all-inside meniscal repair devices appear to decrease risk of neurologic injury (95, 96). The manufacturer’s instructions should be followed to avoid posterior overpenetration. Implants should be directed away from the central portion of the knee posteriorly. Clinical reports of meniscal repair success have not noted any neurologic complications associated with the devices (97, 98, 99, 100 and 101).
PUMP/TOURNIQUET/COMPARTMENT SYNDROME
During arthroscopy, fluid is instilled into the knee under pressure by either a gravity fed inflow or an infusion pump. The infusion pump allows control of both fluid pressure and flow, which is helpful in maintaining hemostasis during the procedure. Under normal circumstances, the use of a pump is not associated with a significant increase in leg compartment pressures (102, 103). Complications are associated with extravasation of fluid. Femoral nerve palsies have been reported after fluid tracked into the thigh with pump pressures between 150 and 300 mm Hg (104). Extravasation leading to thigh and leg compartment syndrome has been associated with pressures as low as 30 mm Hg (105). When the pressure sensor failed, Romero et al. (106) reported extravasation into the scrotum and peritoneum. Fluid has been shown to flow into the thigh through a defect in the suprapatellar pouch and into the leg through a defect in the bursa between the semimembranosis and the gastrocnemius muscles caused by increased pressure (107). The risk is increased in patients with capsular rents associated with tibial plateau fractures or combined ligament reconstruction and high tibial osteotomy procedures (108, 109). If there are no fascial defects in the leg, it has been shown in swine that extravasated fluid dissipates from the compartments quickly and is unlikely to cause ongoing muscle damage (110, 111). Surgeons should be aware of the possibility of fluid extravasation and watch for it. If the compartments are noted to be tense, a brief period of watchful waiting may be warranted before definitive fasciotomy.
The tourniquet is another common means of maintaining hemostasis during knee arthroscopy. Although generally accepted as safe, tourniquet use is associated with a reversible decrease in both muscle and nerve function (112, 113, 114 and 115). Leg compartment syndromes have been attributed to tourniquet use as well (116, 117). Curved and wide cuffs appear to be better tolerated (74). Surgeons are advised to follow the generally accepted advice of limiting tourniquet time to less than 2 hours (77).
Only gold members can continue reading. Log In or Register to continue

 Anthroscopic Cuff Repair: Tissue Graft Applications
Anthroscopic Cuff Repair: Tissue Graft Applications
 Arthroscopic Management of Osteochondritis Dissecans of The Elbow
Arthroscopic Management of Osteochondritis Dissecans of The Elbow
 Arthroscopic Treatment of Dorsal and Volar Ganglions
Arthroscopic Treatment of Dorsal and Volar Ganglions
 Inside-Out and Outside-in Meniscus Repair
Inside-Out and Outside-in Meniscus Repair
 Two-Tunnel Single-Bundle Acl Reconstruction
Two-Tunnel Single-Bundle Acl Reconstruction
 Arthroscopy and Management of Ankle Fractures
Arthroscopy and Management of Ankle Fractures



