Abstract
Objective
To compare the benefits of a thermal cure and non-thermal rehabilitation in treatment of knee osteoarthritis (KOA).
Methods
Randomized therapeutic trial including patients with knee osteoarthritis (American College of Rheumatology criteria). Patients were randomly divided into two groups. Spa treatment consisted of underwater shower, massage-jet showers, hydromassage, pool rehabilitation and peloid therapy. Non-thermal rehabilitation consisted of analgesic physiotherapy, muscle strengthening and group physical rehabilitation. A blinded evaluation was carried out at day 21 and 12 months following treatment. It was based on the visual analogic scale of pain (VAS), which represented the primary endpoint.
Results
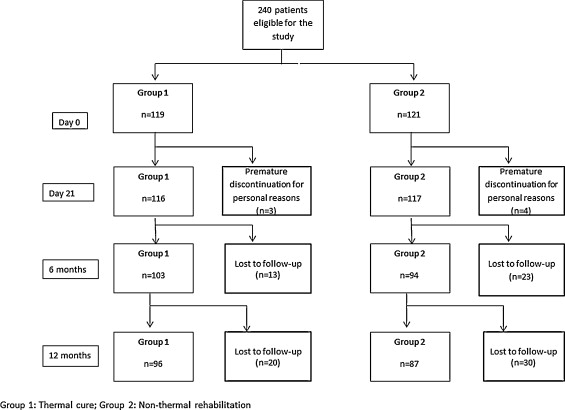
Two hundred and forty patients were included (February–June 2005). The spa treatment and non-thermal rehabilitation groups included 119 and 121 patients respectively. Two hundred and thirty-three patients completed their treatments. Significant improvement of the visual analogic scale of pain was noted in the thermal cure group (61.6 ± 15 at day 0 versus 46.5 ± 22.4 at 12 months, P < 0.001), but not in the non-thermal group (64.1 ± 15 at day 0 versus 62 ± 29 at 12 months, P = 0.68). At day 21, comparison of the two groups revealed no significant difference on the VAS ( P = 0.08). However, at 12 months, the thermal cure group was significantly more improved ( P = 0.000).
Conclusion
In our study, crenobalneotherapy had resulted, at 12 months, in more pronounced long-term improvement of the painful symptoms of KOA than had non-thermal rehabilitation.
Résumé
Objectif
Comparer le bénéfice d’une cure thermale et d’une rééducation à sec sur la gonarthrose.
Méthodes
Essai thérapeutique randomisé portant sur des patients ayant une gonarthrose (critères de l’American College of Rheumatology). Les patients ont été divisés par randomisation en deux groupes. Le traitement thermal comportait des douches sous-marines, douche-massages, hydromassage, rééducation en piscine et application de péloïde chauffée. La rééducation à sec comportait une physiothérapie antalgique, un renforcement musculaire et une rééducation en groupe. Le critère de jugement principal était l’échelle visuelle analogique de la douleur, évaluée en aveugle à j21 et à 12 mois après le traitement.
Résultats
Deux cent quarante patients ont été inclus (février–juin 2005). Le groupe cure thermale comportait 119 patients et le groupe rééducation à sec 121 patients. Deux cent trente-trois patients ont effectué le traitement complet. Une amélioration significative de l’EVA douleur a été notée dans le groupe cure thermale (61,6 ± 15 à j0 versus 46,5 ± 22,4 à 12 mois, p < 0,001) contrairement au groupe rééducation à sec (64,1 ± 15 à j0 versus 62 ± 29 à 12 mois, p = 0,68). À j21, aucune différence significative concernant l’efficacité sur l’EVA douleur n’a été notée en comparant les 2 groupes de traitement ( p = 0,08). À 12 mois par contre, la cure thermale était significativement plus efficace ( p = 0,000).
Conclusion
Notre étude suggère une meilleure efficacité à long terme de la cure thermale sur la composante douloureuse de la gonarthrose comparativement à la rééducation à sec.
1
English version
1.1
Introduction
Osteoarthritis is the most common rheumatic disease. It originates in mechanical and biological phenomena that induce focal alterations of the articular cartilage and subchondral bone remodeling . The knee joint is the most frequent location of osteoarthritis . Its prevalence increases with age . Osteoarthritis entails considerable functional discomfort and impairment because of pain as well as movement limitations that can bring out invalidity or aggravate disability. It represents a major public health problem due to its impact on the quality of life and its substantial socio-economic cost. The objectives of osteoarthritis management are to attenuate pain while improving mobility and the functional capacities of the patient. As non-medical adjuvant treatments, the role of thermal cures is far from clear. Even though the application of thermo-mineral waters or hot springs for therapeutic purposes is a highly ancient and widespread practice in rheumatology, it has up until now been the subject of only a limited number of evaluations and medical publications.
In Tunisia, the history of thermal waters goes back more than two thousand years; during the epoch of the Roman Empire, recourse to hot waters was already current. Tunisian thermal springs are numerous and have traditionally been commercialized as thermal “hammams” and, more recently, as part and parcel of modern medical facilities. The Tunisian office of thermalism estimates that in 2012, 3.3 million spa visitors attended the country’s thermal baths .
In this paper, we report on the results of a randomized therapeutic trial aiming at comparing the benefits, with regard to knee osteoarthritis symptoms, of a thermal cure and a rehabilitative treatment, both of which were conducted in the same spa center on the southern Tunisian island of Djerba.
1.2
Patients and methods
1.2.1
Inclusion criteria
Patients with knee osteoarthritis (KOA) meeting the diagnostic criteria of the American College of Rheumatology (ACR 1992). In addition, KOA had to be symptomatic, as defined by a visual analog scale (VAS) score higher than 30 and by a Lequesne algofunctional index (AFI) score higher than 5.
1.2.2
Exclusion criteria
Subjects presenting with a loss of autonomy necessitating the assistance of another person or with diminished intellectual capacities, as well as those presenting with contraindications to a thermal cure (infectious pathology, poorly controlled hypertension, decompensated cardiopathy, progressive cancer, progressive inflammatory disease, decompensated psychiatric disorder or age greater than 75 years). Other reasons for exclusion were: patients presenting with an inflammatory outbreak of KOA, having recently (within 30 days) undergone intra articular infiltration or suffering from surgical KOA (IAF > 15, walking distance < 1000 m, limitation of flexion to less than 90°), having a rheumatologic disease likely to interfere with measured indices (symptomatic arthropathy of the ankle or the foot, radicular pain) and finally, using stage 3 analgesics (WHO classification).
The baseline visit (D0) took place at least one week before the cure. Selection of the patients who would referred to the spa center was carried out from among the persons consulting at the rheumatology department of Mongi Slim hospital, a Tunis-based university medical center operating independently from the spa center. At that time, the investigating physicians (5 rheumatologists from Mongi Slim hospital and 1 rheumatologist from the spa center in Djerba) verified the inclusion criteria and asked the patients to sign an informed consent form, in its Arabic or French version according to their choices.
All relevant demographic data and clinical history were collected during the initial visit. Finally, anteroposterior and lateral radiographs of the knees were performed in all the patients.
Neither the physicians nor the patients participating in the study were preliminarily informed of the type of treatment to be delivered, whether it was a thermal cure (group 1) or non-thermal rehabilitation (group 2). Choice of type of treatment was determined by the person in charge of the Djerba Care Center, who applied Zelen randomization ; each group was unaware of the existence of another group and of the nature of the treatment to be delivered to the others.
In order to generate a randomization sequence, we established a random list of numbers using the EpiTable program featured in Epi Infoi software (version 6.04d) and assigning treatment 1 to the odd numbers and treatment 2 to the even numbers. Participants were equilibrated following each 20-number sequence. Two groups of 120 patients were thereby constituted. The patients were divided into 7 contingents.
The treatments were given daily in the morning, except on Sundays. Each group sojourned for 20 days in the health care center. Monitoring of management, assiduity and tolerance was performed throughout the cure by the spa center rheumatologist.
Thermal cure and physical rehabilitation were delivered in the Sidi Zikri spa resort, on the Tunisian isle of Djerba, an area at some distance from the patients’ usual places of residence.
The thermal treatment used hot (36 °C), chlorinated water with a slight amount of sodium sulfate as well as calcium and magnesium ( Table 1 ). Everyday, the patients received 4 out of the 5 following treatments: underwater showers (15 minutes), massages-jet showers (10 minutes), hydromassage (20 minutes), pool rehabilitation (20 minutes) and application of heated peloid on the knees (15 minutes).
| Cations | mg/L | Anions | mg/L |
|---|---|---|---|
| Calcium | 340.00 | Bicarbonates | 170.80 |
| Magnesium | 170.24 | Sulfates | 1274.30 |
| Sodium | 1960.00 | Chlorides | 2911.00 |
| Potassium | 56.00 | Fluorides | 0.58 |
| Nitrates | Absent |
Physical rehabilitation treatment was delivered drily and consisted in a classic knee osteoarthritis rehabilitation program, that is to say analgesic electrotherapy (30 minutes) and muscle strengthening, as well as physical rehabilitation group sessions.
The main outcome measure was the Visual Analog Scale (VAS) for pain, which was blindly evaluated for each patient by the same doctor on the final day of the cure (D21) and at 12 months after the end of the cure. Secondary outcome measures were represented by the VAS for pain at 6 months and by the Lequesene AFI score and the WOMAC (Western Ontario and McMaster universities osteoarthritis) index at D21, 6 months and 12 months. In order to calculate the number of subjects needed in a group, we set alpha risk at 0.05, beta risk at 0.20 and minimum clinically significant difference in VAS score between the groups at 20 out of 100. The expected percentage of patients improved by the cure was 50%.
This study received the approval of the ethics committee for therapeutic trials of Mongi Slim hospital.
1.3
Statistical analysis
The data were captured using Epi-Info 1 software (version 2002) and then exported in Dbase III+ ® format before being read and analyzed using SPSS ® version 9.0. Comparison of the means between the two groups at the different times was carried out using the Student’s t -test. Comparison of the percentages was performed using Pearson’s Chi 2 test. As an alternative in case of non-validity, we used Fisher’s exact bilateral test for 2 × 2 tables. The significance level for P was set at 0.05 for the statistical tests.
1.4
Results
1.4.1
The study population
Two hundred and forty patients were included from February 1 through June 30, 2005 and referred to the thermal center of Djerba. The details concerning the respective number of spa patients in the 2 groups who were evaluated at different times for the purposes of the study are summarized in Fig. 1 . The compliance rate came to 80.7% in group 1 and 71.9% in group 2; the difference between the two groups was not significant ( P = 0.11).
The demographic and clinical baseline parameters of the two groups are indicated in Table 2 .
| Group 1 ( n = 119) | Group 2 ( n = 121) | P | |
|---|---|---|---|
| Age (years) | 59.5 ± 8 | 60.3 ± 9 | NS |
| Men/women | 30/89 | 31/90 | NS |
| Weight | 81.1 ± 14 | 85.1 ± 14 | NS |
| Height | 155 ± 7 | 157.2 ± 9 | NS |
| BMI (kg/m 2 ) | 32.5 ± 5.3 | 34.5 ± 5.4 | NS |
| VAS pain | 61.6 ± 14 | 64.3 ± 13 | NS |
| Lequesne index | 11.3 ± 2 | 11.8 ± 3 | NS |
| WOMAC total | 1312 ± 400 | 1279 ± 460 | NS |
| WOMAC pain | 277 ± 86 | 267 ± 84 | NS |
| WOMAC stiffness | 103 ± 40 | 103 ± 39 | NS |
| WOMAC function | 911 ± 274 | 909 ± 313 | NS |
In 55.9% of the cases, KOA was femorotibial, internal, and unilateral. In 67.6% of the cases, KOA was highly advanced, and had reached grade 2 or grade 3 in the Kellgren and Lawrence radiographic classification system .
Once anonymity was lifted, it became known that while 119 patients had undergone a thermal cure, 121 had undergone non-thermal rehabilitation. Not a single patient refused to be part of the group into which he had been randomized.
1.4.2
Tendencies of the clinical indexes after treatment by thermal cure and by non-thermal rehabilitation
In group 1, which comprised the patients treated by thermal cure, a statistically significant improvement in terms of the parameters of evaluation was observed at D21, at 6 months and at 12 months with the exception of the Lequesne indexes at 6 months and at 12 months and of the total WOMAC index at 12 months.
In group 2, which comprised the patients treated by physical rehabilitation, a statistically significant improvement in terms of the parameters of evaluation was observed at D21, at 6 months and at 12 months, with the exception of the VAS for pain at 12 months.
1.4.3
Comparison of the results of the two groups
Comparison of the evaluation parameters according to the two types of tested treatments showed a certain number of statistically significant differences, which are illustrated in Table 3 . The VAS and WOMAC pain scores at 12 months were significantly lower in the thermal cure group, while the Lequesne index and the VAS and WOMAC pain scores at 6 months were significantly lower in the physical rehabilitation group.
| D0 ( n = 240) | D21 ( n = 233) | 6 months ( n = 197) | 12 months ( n = 183) | |
|---|---|---|---|---|
| VAS pain | ||||
| G1 | 61.2 ± 14.3 | 31.5 ± 18.4 | 46.4 ± 23.5 | 46.5 ± 22.4 |
| G2 | 64.1 ± 15 | 27.4 ± 17.1 | 38.6 ± 25.9 | 62 ± 29 |
| P | 0.13 | 0.08 | 0.027 a | 0.000 a |
| Lequesne index | ||||
| G1 | 11.5 ± 2.2 | 2.6 ± 3 | 11.2 ± 3.8 | 10.3 ± 3.8 |
| G2 | 11.8 ± 2.8 | 1.9 ± 2.9 | 9.9 ± 4.8 | 10.4 ± 4.6 |
| P | 0.36 | 0.07 | 0.035 a | 0.87 |
| WOMAC total | ||||
| G1 | 1297 ± 354.8 | 315 ± 297 | 936 ± 482 | 1067.4 ± 1370 |
| G2 | 1279 ± 414 | 452.4 ± 348 | 819 ± 556.7 | 963.8 ± 556.8 |
| P | 0.72 | 0.001 a | 0.11 | 0.51 |
| WOMAC pain | ||||
| G1 | 277 ± 86 | 110.9 ± 96.8 | 197 ± 105 | 189 ± 103 |
| G2 | 267 ± 84.8 | 110 ± 87.4 | 163.8 ± 115.6 | 275.6 ± 84 |
| P | 0.36 | 0.94 | 0.046 a | < 10 −6 |
| WOMAC stiffness | ||||
| G1 | 103 ± 40 | 44.8 ± 43.2 | 78.8 ± 51 | 70.17 ± 47 |
| G2 | 103.7 ± 38 | 44 ± 39 | 66 ± 50 | 79.5 ± 51 |
| P | 0.89 | 0.88 | 0.08 | 0.06 |
| WOMAC function | ||||
| G1 | 911 ± 274 | 339 ± 310 | 664.7 ± 344 | 674 ± 371 |
| G2 | 907.9 ± 314 | 299 ± 236 | 589 ± 402 | 692 ± 406.9 |
| P | 0.94 | 0.27 | 0.16 | 0.75 |
1.5
Discussion
In our study, the results obtained regarding the VAS pain scores and the secondary outcome measures at the end of the cure (D21) were all together comparable in the 2 groups having undergone two different types of treatment.
At 12 months, however, the VAS pain score, which constituted the main outcome measure, was significantly lower in the group 1 than in the group 2. Moreover, the WOMAC pain score was statistically lower at 12 months in the former than in the latter. One may conclude that the thermal treatment had a more pronounced effect on the symptomatic pain component, and that its benefits were confirmed at one year.
Treatment by physical rehabilitation was associated with greater effectiveness on the function and pain components at six months. Indeed, the Lequesne index (AFI) was significantly lower in the physical rehabilitation group than in the thermal cure group, as were the VAS and the WOMAC pain scores. However, at 12 months, this efficacy was not sustained.
Our results differ from those previously reported in the literature. A systematic review of the literature carried out by Forestier et al. came to the conclusion that crenobalneotherapy had a positive therapeutic effect on osteoarthritis of the limbs from a pain-related as well as a functional standpoint . This was equally the case in a multicenter randomized clinical trial (RCT) comparing thermal treatment with physical exercises (195 patients) to physical exercises alone (187 patients), in which significant improvement for the VAS pain score and the WOMAC function component were observed in the thermal group at 6 months . A study with sub-group analysis taking place after the RCT and dealing with KOA in a context of generalized osteoarthritis indicated that a thermal cure associated with home exercises could be of greater value than exercises alone with regard to pain as well as functional capacities .
In a study by Nguyen et al. comparing 91 patients suffering from KOA and treated by means of thermal cure over two successive years to 97 control patients likewise suffering from KOA but carrying on with their usual treatment, an improvement with regard to the Lequesne index, quality of life and the VAS pain score was achieved and maintained at 6 months in the thermal cure group .
While balneotherapy has been cited by the OARSI (the Osteoarthritis Research Society International) as a therapeutic means of KOA and is of proven, it has not been included in the recommendations issued by the ACR or the European League Against Rheumatology (EULAR) . This omission has essentially to do with the difficulty of conducting rigorous clinical trials on therapies not involving drugs. Retrospective and open studies do not methodologically suffice to corroborate the alleged benefits of thermal treatment.
As concerns the analysis grid evaluating the internal validity of non-pharmacological trials (CLEAR grid) , Forestier et al., have underlined their frequently mediocre quality from the standpoint of methodology and/or statistical analysis; as a result, it is not easy to validate the observed differences that would appear to favor balneotherapy .
Moreover, it is particularly difficult to blind patients in placebo-controlled studies. In our study, a certain degree of patient blindness was achieved because randomization involved groups of patients who had no information on the type of treatment applied to the others, which meant that risk of disappointment bias was reduced .
The second difficulty lies in the fact that the benefits of thermal treatment are partially attributed to a “cure effect” brought about by physical repose and a salutary break with the usual environment, while only therapeutic abstention or a home-based medical treatment have been proposed to the control group. Wishing to remedy this difficulty, we have compared the effects of thermal treatments to those of non-thermal physical rehabilitation treatment, with the two types of therapies being delivered at the same center and with the same accommodations being provided for stays of identical duration. In our study, we were indeed able to limit the impact of the “cure effect” with regard to the differences in effectiveness observed in the thermal cure group as opposed to the control group.
Another difficulty is related to the diversified characteristics of the thermal springs (richness in minerals or trace elements, natural radioactivity, heat) and the likewise diversified thermal care protocols. That much said, our protocol was similar to the standard protocols applied in European balneotherapy centers.
A non-comparative method of prolonged observation of a cohort with repeated measurements allows for circumvention or avoidance of the above-mentioned difficulties. In fact, this method is classified in the international literature as a quasi-experimental research design and is applied each time a randomized and blinded method cannot be used given the nature of the treatment to be evaluated, as it is clearly the case with thermal care . Comparative methods with randomization are nevertheless considered as the most conclusive. To our knowledge, our study is the first to have compared thermal to non-thermal physical rehabilitation, both of which had been carried out in the same center.
The interest of some randomized studies may be reduced by a limited number of participants, insufficient critical distancing or recruitment of a sample of non-representative patients. In addition to its prospective nature, our study is distinguished by a consequential scale of participation and the prolonged duration of medical follow-up, which was carried on until 12 months after the end of the cure.
1.6
Conclusion
Our study suggests that a thermal cure has greater effectiveness than non-thermal rehabilitation with regard to the pain component of KOA. On the other hand, the confirmed superiority of physical as opposed to thermal treatment with regard to the function component of KOA suggests the interest of adding, on a track parallel to that of the thermal cure protocol, a rehabilitative program of muscle strength reinforcement that could optimize the results of thermal treatment.
Disclosure of interest
The authors declare that they have no conflicts of interest concerning this article.
2
Version française
2.1
Introduction
L’arthrose est la pathologie rhumatismale la plus fréquente. Elle répond à des phénomènes mécaniques et biologiques qui induisent des altérations focales du cartilage articulaire et des remaniements de l’os sous-chondral . L’articulation du genou est la localisation arthrosique la plus fréquente . Sa prévalence augmente avec l’âge . L’arthrose entraîne une gêne fonctionnelle importante, en raison de la douleur et de la limitation des mouvements, responsable d’une invalidité ou d’un handicap surajouté. Elle constitue un problème majeur de santé publique en raison de son impact sur la qualité de vie et de son coût socioéconomique élevé. La prise en charge de l’arthrose a pour objectif d’atténuer la douleur et d’améliorer la mobilité ainsi que les capacités fonctionnelles des patients. Parmi les traitements adjuvants non médicamenteux, la place du thermalisme n’est pas claire. En effet, même si l’utilisation d’eaux thermo-minérales à des fins thérapeutiques est une pratique très ancienne et répandue en rhumatologie, elle n’a fait l’objet que d’un nombre relativement limité d’évaluations et de publications médicales.
En Tunisie, l’histoire des eaux thermales remonte à plus de deux mille ans et le recours aux eaux chaudes était déjà d’usage à l’époque romaine. Les sources thermales tunisiennes sont nombreuses et font l’objet d’une exploitation traditionnelle dans le cadre de « hammams » thermaux ou plus récemment dans des centres modernes et médicalisés. L’office tunisien du thermalisme estime que 3,3 millions de curistes ont fréquenté des bains thermaux au cours de l’année 2012 .
Nous rapportons les résultats d’un essai thérapeutique randomisé, réalisé dans le but de comparer le bénéfice, sur les symptômes de la gonarthrose, d’une cure thermale et d’un traitement rééducatif conduit à sec dans le même centre thermal, situé sur l’île sud tunisienne de Jerba.
2.2
Patients et méthodes
2.2.1
Critères d’inclusion
Patients présentant une gonarthrose répondant aux critères diagnostiques de l’American College of Rheumatology (ACR 1992). De plus, la gonarthrose devait avoir un caractère symptomatique défini par une échelle visuelle analogique (EVA) douleur supérieure à 30 et un indice algofonctionnel (IAF) de Lequesne supérieur à 5.
2.2.2
Critères d’exclusion
Les sujets présentant une perte d’autonomie, nécessitant en particulier l’aide d’une tierce personne, ceux dont les capacités intellectuelles étaient diminuées ainsi que ceux présentant des contre-indications à la cure thermale (pathologie infectieuse, hypertension artérielle mal équilibrée, cardiopathie décompensée, cancer évolutif, pathologie inflammatoire évolutive, maladie psychiatrique décompensée ou âge supérieur à 75 ans). Ont également été exclus les patients présentant une gonarthrose en poussée congestive, ayant bénéficié d’une infiltration intra-articulaire récente (moins de 30 jours), une gonarthrose au stade chirurgical (IAF > 15, périmètre de marche < 1000 m, limitation de la flexion à moins de 90°), la présence d’une affection rhumatologique susceptible d’interférer avec les indices mesurés (arthropathie symptomatique de la cheville ou du pied, douleur radiculaire) et enfin l’utilisation d’antalgiques de palier III de l’OMS.
La visite d’inclusion (j0) a été effectuée au plus tard une semaine avant la cure. La sélection des patients à adresser au centre thermal a été réalisée à partir des malades consultants du service de rhumatologie de l’hôpital Mongi Slim, centre hospitalo-universitaire de la capitale indépendant du centre thermal. Les médecins investigateurs (5 rhumatologues de l’hôpital Mongi Slim et 1 rhumatologue du centre thermal de Jerba) ont à cette occasion vérifié les critères d’inclusion et ont fait signer le consentement éclairé, en version française ou arabe selon le choix des patients.
Toutes les données démographiques et l’histoire clinique ont été également recueillies lors de cette première visite. Des radiographies des genoux en charge, de face et de profil, ont été pratiquées chez tous les patients.
Ni les médecins participant à l’étude ni les patients n’étaient informés préalablement du type de traitement qui sera délivré, cure thermale (groupe 1) ou rééducation à sec (groupe 2). Celui-ci a été déterminé par méthode de randomisation assuré par le responsable du centre de soin de Jerba selon la méthode de Zelen ; chaque groupe ignorant l’existence de 2 groupes de randomisation et la nature du traitement délivré aux autres.
Pour générer la séquence de randomisation, nous avons établi une liste de nombres au hasard au moyen du programme Epitable du logiciel Epi Infoi version 6.04d, en attribuant le traitement 1 aux nombres impairs et le traitement 2 aux nombres pairs, et en équilibrant les effectifs à chaque séquence de 20 nombres. Deux groupes de 120 patients chacun ont été constitués. Les patients ont été divisés en 7 contingents.
Les traitements ont été délivrés quotidiennement, le matin, à l’exception des dimanches. Chaque groupe a séjourné durant 20 jours dans le centre de soin. Le suivi du déroulement des soins, de l’assiduité et de la tolérance lors de la cure a été effectué par le rhumatologue du centre thermal.
Le traitement thermal et le traitement par rééducation physique ont été délivrés dans la station thermale de Sidi Zikri, sur l’île tunisienne de Jerba, ville éloignée du lieu de résidence habituel des patients.
Le traitement thermal utilisait une eau chaude (36°), chlorurée, sodique et légèrement sulfatée, calcique et magnésienne ( Tableau 1 ). Les patients ont reçu quotidiennement 4 parmi les 5 soins suivants : douches sous-marines (15 minutes), douche-massages (10 minutes), hydromassage (20 minutes), rééducation en piscine (20 minutes) et application de péloïde chauffée sur les genoux (15 minutes).
Related posts:
 Enhancing Annalsvalue through quality
Enhancing Annalsvalue through quality
 Detection of progressive idiopathic scoliosis during growth using back surface topography: A prospective study of 100 patients
Cognitive and behavioural post-traumatic impairments: What is the specificity of a brain injury ? A study within the ESPARR cohort
Detection of progressive idiopathic scoliosis during growth using back surface topography: A prospective study of 100 patients
Cognitive and behavioural post-traumatic impairments: What is the specificity of a brain injury ? A study within the ESPARR cohort
 Quality of life and satisfaction after multilevel surgery in cerebral palsy: Confronting the experience of children and their parents
Quality of life and satisfaction after multilevel surgery in cerebral palsy: Confronting the experience of children and their parents
 Communication disorders and executive function impairment after severe traumatic brain injury: An exploratory study using the GALI (a grid for linguistic analysis of free conversational interchange)
Communication disorders and executive function impairment after severe traumatic brain injury: An exploratory study using the GALI (a grid for linguistic analysis of free conversational interchange)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


