Chapter 37 Common Neck Problems
Introduction and Epidemiology
Successful treatment of painful cervical spinal disorders hinges on the accurate assessment of the underlying tissue injury, which can involve a broad range of biomechanical and biochemical disorders. The clinician needs to conceptualize a process of diagnosis and treatment that incorporates an understanding of the pathophysiology of cervical spine injury and the associated potential symptom manifestations, an awareness of the advantages and disadvantages of the myriad of diagnostic tools, and a knowledge of the potential therapeutic options. The initial step in this process is the history taking. It is important that one distinguish between cervical axial pain (neck pain) and upper limb pain. As eloquently stated by Bogduk,25 the neck is not the upper limb, and the upper limb is not the neck. Pain in the upper limb is not pain in the neck, and vice versa.
Cervical axial pain must not be mistaken for cervical radicular pain. Cervical axial pain is defined as pain occurring in all or part of a corridor extending from the inferior occiput inferiorly to the superior interscapular region, localizing to the midline or just paramidline. The patient perceives it as stemming from the neck. Cervical radicular pain, defined as pain involving the shoulder girdle, distal areas or both, manifests as pain in the upper limb. The etiologies of these two different sets of symptoms vary, as does the diagnosis and management of each. Equating cervical axial and cervical radicular pain can result in misdiagnosis, inappropriate investigation, and institution of suboptimal treatment.25 Such confusion can easily occur because both disorders result from injury to the cervical spine. Each of these injuries or conditions differs in occurrence, mechanism, pathophysiology, treatment, and rehabilitation.
Epidemiologic reports have sometimes clustered neck and limb pain, but neck complaints are ubiquitous. The prevalence of neck pain with or without upper limb pain ranges from 9% to 18% of the general population,130,145,238,248 and one of three individuals can recall at least one incidence of neck pain in their lifetime.130 Cervical pain is more frequently encountered in clinical practice than is low back pain,256 and traumatic neck pain becomes chronic in up to 40% of patients, with 8% to 10% experiencing severe pain.55 The occurrence increases in the workplace, with a prevalence of 35% to 71% among Swedish forest and industrial workers.98,99 The frequency of occupational cervical complaints increases with age. Approximately 25% to 30% of workers younger than 30 years report neck stiffness, and 50% of workers older than 45 years report similar complaints.100,238,248
Cervical radiculopathy occurs less commonly, with an annual incidence of 83.2 per 100,000, and peaks at 50 to 54 years of age.187 Five to ten percent of workers younger than 30 years complain of pain referring into the upper limb, whereas 25% to 40% of those older than 45 years experience pain in the upper limb.100 Overall, 23% of working men have experienced at least one episode of upper limb pain.100 Neck pain, cervical radicular pain, or both are common complaints across different patient profiles.
Pathophysiology and the Significance of Pain Referral Patterns
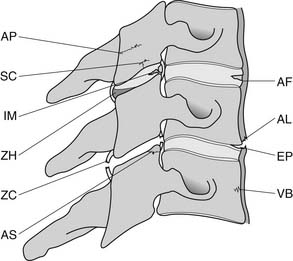
A working knowledge of the anatomic interrelationships within the cervical spine (Figure 37-1) is important, to comprehend the pathomechanisms of cervical spine disorders. The cervical spine is a discrete segment of the axial skeleton (see Figure 37-1), and functions to support and stabilize the head; allow the head to move in all planes of motion; and protect the spinal cord, nerve roots, spinal nerves, and vertebral arteries.163 There are seven cervical vertebrae and eight cervical nerve roots. The atlantooccipital (C0–1) articulation permits 10 degrees of flexion and 25 degrees of extension. The C1–2 level or the atlantoaxial joint (Figure 37-2) forms the upper cervical segment and is responsible for 40% to 50% of all cervical axial rotation, demonstrated clinically by 45 degrees of rotation in either direction.61,62,65,70,249 Below the C2–3 level, lateral flexion of the cervical spine is coupled with rotation in the same direction. This spinal segment marks a transition where permitted motion changes from rotation to flexion, extension, and lateral bending.70,242 This combined motion is facilitated by the 45 degrees sagittal inclination of the cervical zygapophyseal joints (see Figure 37-1).147 The zygapophyseal joints allow motion within the cervical spine, connect each vertebral segment,216 and are innervated by medial branches from the cervical dorsal rami (Figure 37-3).21 In addition, the C0–1 joint is innervated by the C1 ventral ramus,122 and the C1–2 joint by the C2 ventral ramus laterally131 and the sinuvertebral nerves of C1, C2, and C3 medially.120 The greatest amount of flexion occurs at C4–5 and C5–6, while lateral bending occurs primarily at C3–4 and C4–5.70,242 The lower cervical vertebrae (C3–7) have unique synovial joint-like articulations, uncovertebral joints or joints of Luschka, located between the uncinate processes (Figure 37-4).165 These joints commonly develop osteoarthritic changes, which can narrow the diameter of the intervertebral foramina (Figure 37-5).80,97,234 These intervertebral foramina are widest at the C2–3 level and progressively decrease in size to the C6–7 level. The radicular complex of dorsal root ganglia, nerve roots, spinal nerve, and surrounding sheath accounts for 20% to 35% of the cross-sectional area of the intervertebral foramina.80,97,234 The remaining intervertebral foramina volume is filled by loose areolar or adipose tissue, Hoffman’s ligaments, radicular artery, and numerous venous conduits that usually encircle the nerve roots.216 The neuroforamina are bordered anteromedially by the uncovertebral joint, superiorly and inferiorly by successive pedicles, and medially by the edge of the vertebral end plate and intervertebral disk (see Figure 37-5).216
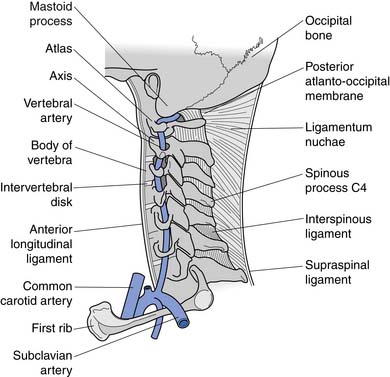
FIGURE 37-1 Anatomic relationship of cervical spine ligaments to other structures in the neck.
(Redrawn from Crafts RC: Textbook of Human Anatomy, ed 2, New York, 1979, John Wiley.)
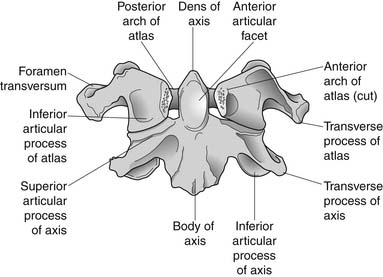
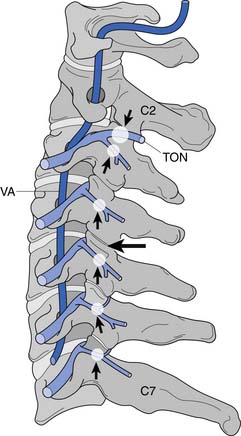
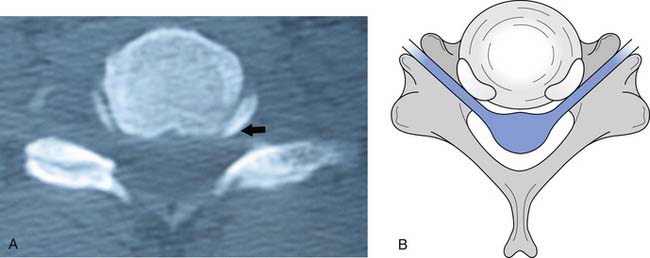
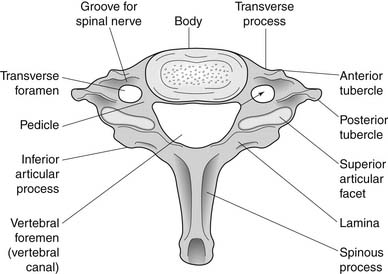
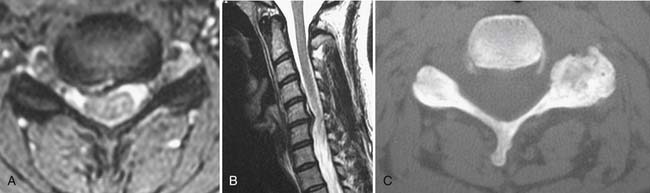
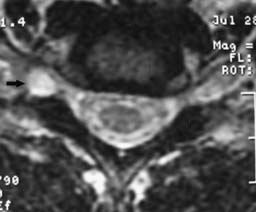
FIGURE 37-5 Axial view of the seventh cervical vertebrae, illustrating the intervertebral foramen (black arrow).
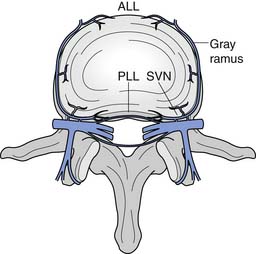
The intervertebral disks are located between the vertebral bodies of C2 through C7. Each is composed of an outer annulus fibrosis innervated posterolaterally by the sinuvertebral nerve, comprising branches from the vertebral nerve and ventral ramus, and innervated anteriorly by the vertebral nerve (Figure 37-6).30 The inner portions of the disks comprise the gelatinous nucleus pulposus, providing transmission of axial loads to dissipate forces throughout various ranges of motion.216 Each intervertebral disk is thicker anteriorly than posteriorly, which contributes to the natural cervical lordotic curvature.216 Normal cervical spine anatomy can undergo degenerative or traumatic changes, leading to various cervical spine disorders.
Three essential requirements are needed for a structure to serve as a source of pain. It must be innervated, capable of producing pain similar to that seen clinically, and susceptible to disease or injury known to be painful.23 Nonneural structures of the neck, such as the intervertebral disk, zygapophyseal joint, posterior longitudinal ligament, and muscles, can serve as a nidus for pain and produce somatic referral of pain into the upper limb.38,69,116–118,128 Classic experiments have demonstrated that stimulation of these posterior midline structures produces local neck pain as well as somatically referred pain into the upper limb.38,69,116–118,128 Kellegren117,118 was first to investigate the pain referral patterns of nonneural spinal structures by stimulating periosteum, fascia, tendon, and muscle with hypertonic saline. He hypothesized that a central nervous system phenomenon mediated the pain referral, because anesthetizing the corresponding peripheral nerve distal to the site of stimulation did not diminish the distally referred pain. These experiments were the first to demonstrate this phenomenon of somatically referred pain, and that cervical spinal disorders could produce pain in the upper limb as well as headache.38,69,116–118,128 These symptoms were produced without irritation of neural tissue. Such pain referral has been termed somatic, previously labeled as sclerotomal, and occurs when a mesodermal structure such as a ligament, joint capsule, intervertebral disk annulus, or periosteum is stimulated, leading to symptoms referred into another mesodermal tissue structure of similar embryonic origin.216 This mechanism of somatically referred symptoms involves convergence.25 Afferents from both the cervical spine and the distal upper limb converge on second-order neurons within the spinal cord, allowing spinal pain to be misperceived as arising from those distal limb sites.25 It is via this mechanism that cervical intervertebral disks and zygapophyseal joints create upper limb symptoms.216
It is thought that biomechanical and/or biochemical insults to nonneural structures can trigger nociceptive nerve fibers, via compression or inflammation, causing pain referral.216 Mechanical stimulation of the cervical zygapophyseal joints or their innervating nerves has been shown to produce head and neck pain with upper limb referral patterns (Figure 37-7).10,59,63,73 Anesthetizing symptomatic joints has revealed similar patterns of symptomatic referral from the cervical joints.28,219
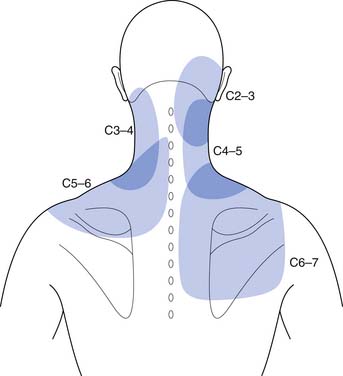
FIGURE 37-7 Pain referral from C2–C3 through C6–C7 facet joints.
(Redrawn from Dwyer A, Aprill C, Bogduk N: Cervical zygapophyseal joint pain patterns. I: A study in normal volunteers, Spine 15:453-457, 1990, with permission.)
Pain emanating from the cervical zygapophyseal joints tends to follow relatively constant and recognizable referral patterns. The C1–2 and C2–3 levels refer rostrally to the occiput. The C3–4 and C4–5 joints produce symptoms over the posterior neck. Pain from the C5–6 joint spreads over the supraspinatus fossa of the scapula, whereas pain from the C6–7 joint spreads further caudally over the scapula.∗ Additionally, C1–2, C2–3, C3–4, and C4–5 zygapophyseal joints can refer pain to the face, and C3–4, C4–5, and C5–6 can refer symptoms to the head.28 Each joint can produce unilateral or bilateral symptomatology. It is not intuitive that a unilateral joint could trigger only contralateral pain, and this manifestation has never been formally investigated.218
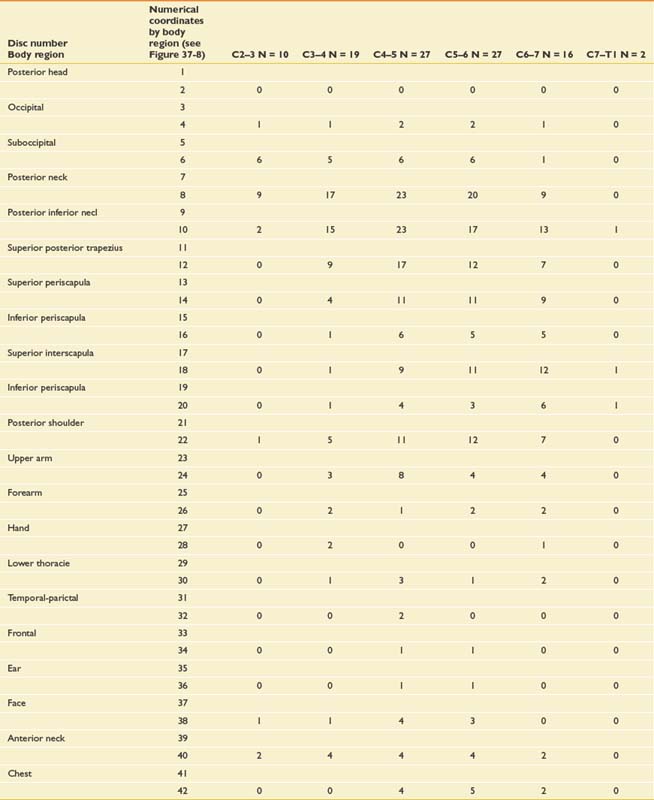
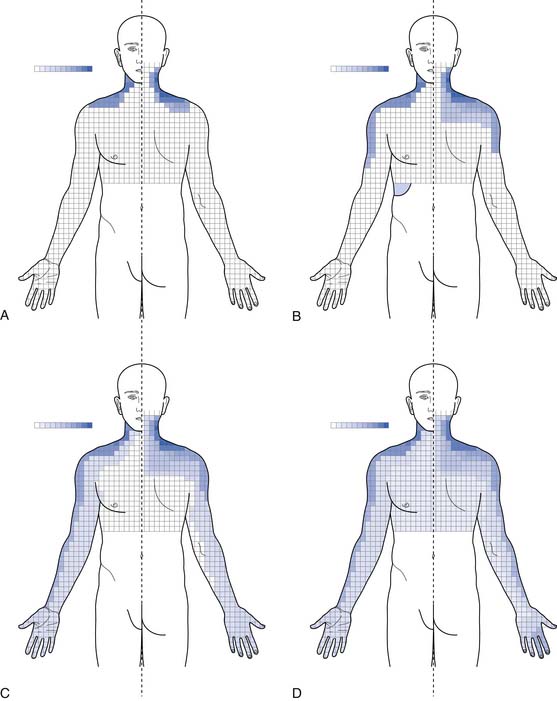
Very similar pain patterns have been produced by mechanical stimulation of the cervical intervertebral disks (Figure 37-8 and Table 37-1).45,78,203,224 In our experience, bilateral paramidline upper neck pain without associated headaches is commonly caused by cervical intervertebral disk disruption (CIDD) rather than zygapophyseal joint–mediated pain. Our observations are supported by Grubb and Kelly’s recent study78 that found that 34% to 50% of cervical disks produced bilateral pain at each cervical disk level. Furthermore, a more detailed study from the Penn Spine Center revealed that 30% to 62% of cervical disks produced bilateral pain during cervical discography.224 When taken together, these findings support the notion that the pattern of pain stemming from a particular structure is a consequence of that structure’s innervation rather than the structure itself.25 In line with this logic is the finding that stimulation of the upper cervical musculature can produce pain in the head.52 Discriminating CIDD-mediated pain from zygapophyseal joint pain or pain emanating from the cervical spine soft tissues requires systematic and meticulous interpretation of history and physical examination findings.
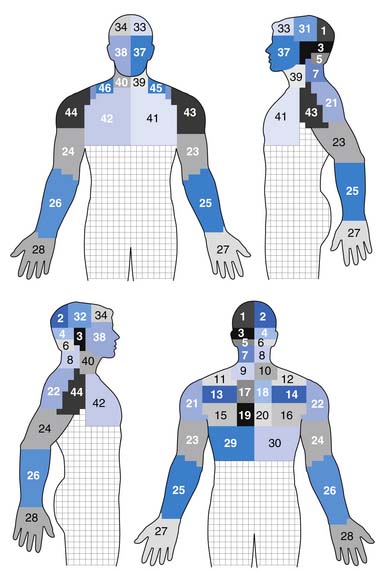
FIGURE 37-8 Pain referral patterns from cervical intervertebral discs stimulated during cervical provocation discography. Pain referral into each area demarked by a number was recorded during disc stimulation (see Table 37-1).
(Redrawn from Slipman CW, Plastaras C, Patel R, et al: Provocative cervical discography symptom mapping, Spine J 5[4]:381-388, 2005, with permission.)

Cervical radicular pain is a fundamentally different clinical picture because the presenting chief complaint is typically upper limb pain more severe than axial pain. The etiology of upper limb symptoms can be confusing when a nonradicular disorder creates symptoms in a radicular distribution, or when a usually radicular disorder causes pain in an uncharacteristic dynatomal pattern (dynatomal pattern—pattern of referred symptoms).225 Regardless, radicular pain is most consistent with upper limb symptoms that are more intense than axial complaints.216 Upper limb pain caused by cervical radiculopathy can refer symptoms into the arm, forearm, and/or hand (Figure 37-9).64 However, periscapular or trapezial pain greater than neck pain can be caused by upper cervical nerve root involvement such as C4 or C5.225 Radicular pain from C5 tends to remain in the arm, but pain from C6, C7, and C8 extends into the forearm and hand. Nevertheless, pain that is primarily in the upper back with or without arm symptoms can emanate from the C4 through C6 roots. When experienced in the middle to lower aspect of the ipsilateral scapula, the C7 or C8 roots could be the culprit.
Nerve vulnerability within the intervertebral foramina arises consequent to changes in one or more of three separate structures: the zygapophyseal joints, the uncovertebral joints, and the intervertebral disk. The most common cause of cervical radiculopathy is a herniated cervical intervertebral disk,102 followed by cervical spondylosis259 with or without cervical myelopathy (Box 37-1). The precise mechanism by which disk herniation or spondylosis causes radicular pain is still somewhat unclear. Direct neurocompression of the nerve root does not necessarily cause pain,96 and pure myotomal weakness can occur.137 Proposed mechanisms for pain in cervical radiculopathy include nerve root inflammation,25 increased discharge of the dorsal root ganglion, mechanosensitivity or chemosensitivity of the nerve root itself, or direct pressure on chronically injured axons or on a normal dorsal root ganglion.96,189 Other potential causes of cervical radiculopathy include tumor,245 trauma,182 sarcoidosis,11 arteritis,200 and athetoid or dystonic cerebral palsy.72
BOX 37-1 Disorders Affecting the Neck
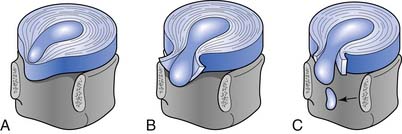
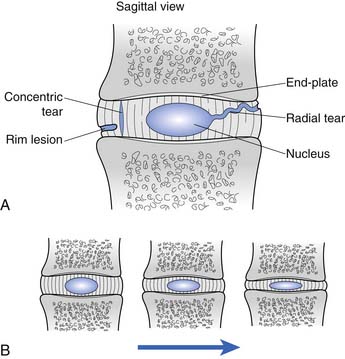
Cervical intervertebral disk injury can be categorized into two broad categories: internal disruption and herniation. Disk herniation is a generalized term, which is further divided into protrusion, extrusion, and sequestration (Figure 37-10). A more thorough discussion of disk herniation follows. Internal disk disruption is a descriptive phrase used to detail derangement of the internal architecture of the nucleus pulposus and/or annular fibers with little or no external deformation.51 The process of disk degeneration occurs over a spectrum of disk abnormalities (Figure 37-11). Initially, circumferential outer annular tears secondary to repetitive microtrauma are associated with interruption in blood and nutritional supply to the disk. These tears eventually coalesce to form radial tears occurring concurrently with a decrement in the water-imbibing ability of the nucleus pulposus. The mechanical integrity of the intervertebral disk suffers as the disk space narrows, more tears develop, and type 2 proteoglycans continue to degrade.121 Biochemical insults have been purported to occur before these biomechanical alterations.198 The end result is a cervical disk that is biomechanically incompetent and prone to biochemical insult.
Cervical zygapophyseal joint injury can occur because of osteoarthritis or trauma resulting from both macrotraumatic and microtraumatic events. Acceleration-deceleration zygapophyseal joint injuries can result in osseous injury to the articular pillars, articular surface, or subchondral bone; intraarticular hemarthrosis; contusion of the intraarticular meniscus; or tears of the zygapophyseal joint capsule (Figure 37-12).∗ We have successfully treated patients with cervical zygapophyseal joint synovitis, who had experienced the onset of symptoms on awakening after sleeping in an awkward position. Painful cervical zygapophyseal joint arthropathy can result as a consequence of cervical intervertebral disk degeneration as well. Biochemical and biomechanical effects can both cause cervical zygapophyseal joint symptom manifestation.
Common Clinical Disorders
Cervical Strain and Sprains
Epidemiology
A cervical strain is a musculotendinous injury produced by an overload injury resulting from excessive forces imposed on the cervical spine.48 In contrast, cervical sprains are overstretching or tearing injuries of spinal ligaments. Muscular strains are seen most frequently because many cervical muscles do not terminate in tendons, but rather attach directly to bone via myofascial tissue that blends seamlessly with periosteum.183 Cervical sprain and strain injuries account for approximately 85% of neck pain resulting from acute, repetitive, or chronic neck injuries.105 These injuries are the most common type of injury to motor vehicle occupants in the United States,185 and are one of the most common causes of pain after noncatastrophic sports injuries.48 Approximately one third of individuals involved in motor vehicle collisions develop neck pain within 24 hours of the injury.207 Automobile-related cervical strain and sprain injuries are more common in Western societies and in metropolitan areas having higher densities of motor vehicles.233 The incidence is higher in women and individuals aged 30 to 50 years.233
Pathophysiology
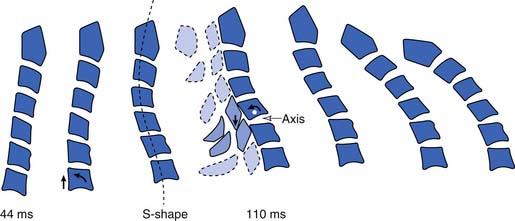
Differing pathomechanisms are causal in cervical strain and sprain injuries, depending on the nature of the abnormal stress applied to the cervical spine. Acceleration-deceleration injuries result in excursions of the cervical spine that result in an S-shaped curvature approximately 100 ms after a rear-end impact.113 By 200 to 250 ms after impact, the head initiates forward flexion of the neck after maximally extending to approximately 45 degrees.154 Posterior neck muscle activation occurs by 90 to 120 ms237 and coincides with the deceleration of the head moving forward.154 As the head continues to move forward, the neck extensors eccentrically contract to decelerate the head, placing them at increased risk for injury (Figure 37-13).168 These experimental findings lend support for a simple muscle or ligamentous strain injury during motor vehicle collisions. Partial and complete muscle tears and hemorrhage have been visualized by ultrasound151 and magnetic resonance imaging (MRI),180 and observed in postmortem examinations.110 Tears of the anterior longitudinal ligament have been reported in surgical explorations34 and identified at postmortem.33 Anatomic studies have demonstrated that the anterior longitudinal ligament merges imperceptibly with the intervertebral disks and can be injured with injury to the cervical disk.190
Physiologic forces acting on a relatively normal cervical spine result in typical soft tissue strain seen in nonathletes. In individuals with thoracic kyphosis and consequential cervical lordosis and extension, strain occurs in the levator scapulae, superior trapezius, sternocleidomastoid, scalene, and suboccipital muscles.48 Traumatic blows often incurred in sporting injuries can result in a more acute cervical strain or sprain.48 Repetitive motions, as occur in recreational activities, can tax shortened and deconditioned cervical rotators, extensors, and lateral flexors that are frequently present in those with cervical spondylosis.48
Diagnosis
Further diagnostic testing such as imaging or electrodiagnostic evaluations are not indicated unless neurologic or motor abnormalities are detected, or significant pain into the limbs is reported. Plain radiography would be ordered first to evaluate for bony malalignment or fractures. It is reasonable to examine cervical flexion and extension radiographs to evaluate for instability before prescribing functional restoration. In most instances these images are normal or reveal nonspecific loss of cervical lordosis because of muscle splinting (Figure 37-14).

Treatment
Physical modalities such as massage, superficial and deep heat, electrical stimulation, and a soft cervical collar can be used in the treatment program. Light massage causes sedation, reduction of adhesions, muscular relaxation, and vascular changes (see Chapter 20)255 Superficial heat133 and deep heat with ultrasound67 produce analgesia and muscle relaxation, help resolve inflammation, and increase connective tissue elasticity (see Chapter 21).192 Transcutaneous electrical nerve stimulation (TENS) can also be effective in modulating musculoskeletal pain (see Chapter 22).146 A soft cervical collar (Figure 37-15) can be prescribed to ease painful sleep disturbances and reduce further neck strain. The collar can be worn while awake, but should be restricted to the first 72 hours after the injury to minimize interference with healing and prevent development of soft tissue tightening.156 A gradual return to activities should be initiated by 2 to 4 weeks after injury, and should include a functional restoration program to address postural reeducation and functional biomechanical deficits.48
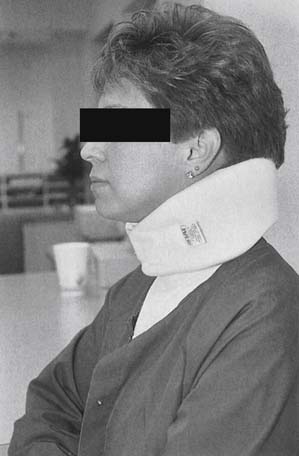
FIGURE 37-15 Cervical orthosis. A cervical soft collar with the widest side posteriorly and the narrowest side anteriorly.
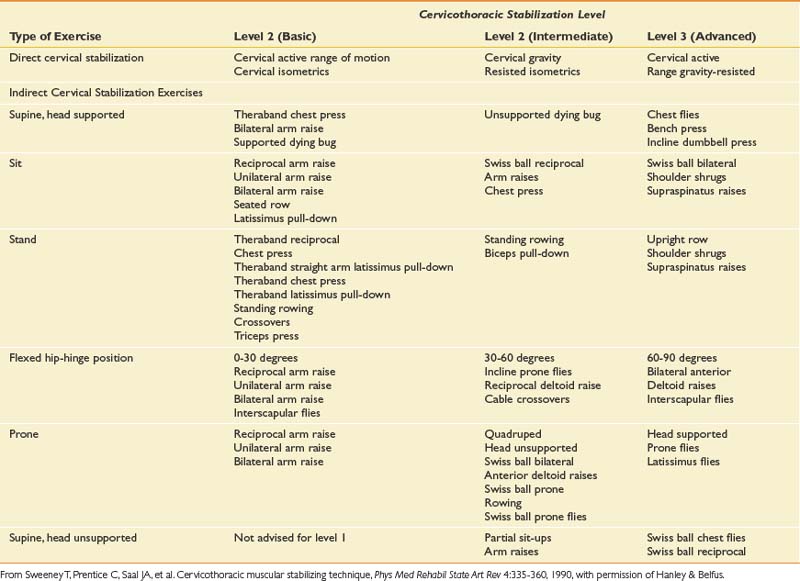
Once the acute pain has improved, proper spinal biomechanics must be restored with the establishment of proper movement patterns. Healthy cervical segmental motion requires efficient stabilization throughout the cervical and thoracic spines. Proprioceptive retraining, balance, and postural conditioning should be incorporated into the exercise regimen. Flexibility and range of motion are improved by mobilization and stretching exercises. Proprioception is improved by using visual feedback during exercises and functional tasks. These should be performed with simultaneous dynamic demands on the patient’s base of support.48,124 Such a program (Table 37-2) enhances the healthy dissipation of forces across the cervical spine with efficient myofascial efforts.
Cervical Radiculopathy and Radicular Pain
Epidemiology
Cervical radiculopathy is a pathologic process involving neurophysiologic dysfunction of the nerve root.64 Signs and symptoms of cervical radiculopathy include myotomal weakness, paresthesias, sensory disturbances, and depressed muscle stretch reflexes.64 Cervical radicular pain represents a hyperexcitable state of the affected nerve root. Cervical radiculopathy, on the other hand, involves reflex and strength deficits marking a hypofunctional nerve root as a result of pathologic changes in nerve root function.25 Separating cervical radicular pain from cervical radiculopathy is important, because treatment strategies will vary depending on the presence or absence of the two conditions.
A large epidemiologic study of 561 patients in Rochester, Minnesota, found an average annual age-adjusted incidence of cervical radiculopathy of 83.2 per 100,000.187 The peak incidence occurred between the ages of 50 and 54 years in the study cohort.187 A history of trauma or physical exertion preceding the onset of symptoms occurred in just under 15% of patients.187 The order of decreasing frequency of involved levels was C7, C6, C8, and C5.187
Pathophysiology
Cervical nerve root injury is most commonly caused by cervical intervertebral disk herniation (CIDH),102 with spondylitic spinal changes the next most common cause (Figure 37-16).167,259 The causal role of neural compression in CIDH-induced radiculopathy was first introduced by Semmes and Murphey208 in 1943. Subsequent radiologic studies have demonstrated the existence of asymptomatic cervical disk abnormalities.20,152,157,240 A growing body of evidence has emerged attesting to the etiologic role of an inflammatory response to a CIDH in some way triggering painful radicular signs and symptoms.74,114,115 Animal studies have shown disrupted nerve root physiology caused by gradient pressure197 and inflammation in the absence of compression.172 Nerve roots are anatomically less resilient than peripheral nerves to both biomechanical and biochemical insults, and respond to each with the same pathologic sequence of events.166
Cervical spondylosis (or degenerative osteoarthritic changes) is manifested by ligamentous hypertrophy, hyperostosis (bony overgrowth), disk degeneration, and zygapophyseal joint arthropathy.259 Hypertrophy of the zygapophyseal joints and uncovertebral joints results in intervertebral foramina stenosis and nerve root impingement.216,259 Vertebral body osteophytes and disk material can form a “hard disk” that can also compress the adjacent nerve root.187,259 Although cervical zygapophyseal joint cysts are rare,142 patients with cervical zygapophyseal joint-induced radiculopathy have been treated at the Penn Spine Center (Figure 37-17). In these cases it is not clear to what extent biochemical versus biomechanical influences affect the neural elements.
Diagnosis
History and Physical Examination
Patients with acute CIDH-related radiculopathy typically report a history of axial cervical pain that is then followed by an explosive onset of upper limb pain. In contrast, spondylitic radicular pain presents more gradually. Cervical radicular pain can masquerade as a deep dull ache or sharp lancinating pain. It can occur in a number of locations, including the medial scapular edge (C5, C6, or C7), superior trapezius (C5 or C6), precordium (C5 or C6), deltoid and lateral arm (C5 or C6), posteromedial arm (C7, C8, or T1), anterolateral forearm (C6 or C7), posterior forearm (C7 or C8), and any of the upper extremity digits (C6, C7, C8, or T1).64,225
Exacerbating factors include activities that raise subarachnoid pressure, such as coughing, sneezing, or Valsalva maneuvers. If a significant component of stenosis is present, cervical extension can amplify the symptoms. Alleviation of the radicular pain by elevating the ipsilateral humerus is known as the shoulder abduction relief sign, which aids in the diagnosis and can be used as a therapeutic manuever.54,68
The physical examination begins with the clinical observation of neck position, as patients characteristically tilt toward the side of the disk herniation. Atrophy can be detected with more severe or longstanding lesions. Muscle wasting in the suprascapular or infrascapular fossae or deltoid suggests C5 or C6 involvement; muscle wasting in the triceps, C7 injury; in the thenar eminence, C8 injury; and in the first dorsal interossei, T1 injury.187 Manual muscle testing has greater specificity than reflex or sensory abnormalities (Table 37-3),257 and might need to be performed repetitively or with the muscle at a mechanical disadvantage to elicit subtle weakness. Severe weakness (<3/5 Medical Research Council [MRC]) is less consistent with a single root lesion and should alert the clinician to the presence of a possible multilevel radiculopathy, α motor neuron disease, plexopathy, or focal peripheral neuropathy. Sensation to light touch, pinprick, and vibration can be altered. The patient should be assessed for the presence of long tract signs such as Hoffman’s sign and Babinski’s response to ensure that there is no spinal cord involvement.
Table 37-3 Nerve Root Levels, Peripheral Nerves, and Muscles of the Upper Limb Commonly Evaluated in the Patient With Neck Pain
| Nerve Root Level | Nerve | Muscle |
|---|---|---|
| C5, C6 | Axillary | Deltoid |
| C5, C6 | Musculocutaneous | Biceps brachii |
| C5, C6 | ||
| C7 | ||
| C8, T1 |
Provocative maneuvers such as neuroforaminal closure and root tension signs help localize the lesion to the cervical spine. Spurling’s maneuver,231 cervical extension, lateral flexion, and ipsilateral axial rotation reproducing radicular symptoms are highly specific but not sensitive for cervical radiculopathy.246 Nerve root tension, contralateral cervical axial rotation concurrent with ipsilateral glenohumeral abduction/extension with elbow and wrist extension, can help detect radicular pain. If this examination reveals radicular pain, presumably the imposed neural tension is provocative as a result of nerve root inflammation. Root tension–induced radicular pain might be more sensitive than Spurling’s maneuver but less specific,195 and should be performed bilaterally to ensure absence of contralateral symptoms. Systematic studies comparing the utility of these two examination maneuvers have not been published. L’hermitte’s sign,13526 which is rapid passive cervical flexion while the patient is seated, can produce an electric shock sensation down the spine and occasionally into the limbs in patients with cervical cord involvement as a result of tumor, spondylosis, or multiple sclerosis.176
Imaging Studies
Although plain cervical radiography is not very sensitive in detecting disk pathology, it remains the initial radiographic examination in almost every assessment of musculoskeletal injury.163 Plain films of anteroposterior, lateral, open mouth, and flexion and extension views are indicated to evaluate spinal stability in cases of rheumatoid arthritis or ankylosing spondylitis,64 spondylolisthesis, after fusion, or after traumatic injury.163 Computed tomographic myelography is regarded as the criterion standard against which other imaging modalities ought to be judged in evaluating degenerative cervical spine conditions.196 However, most clinicians reserve unenhanced computed tomography (CT) for the evaluation of osseous details such as foraminal stenosis,163 bone tumors, and fractures.112
MRI is the imaging modality of choice in investigating cervical radiculopathy,112,150 because it details diskal, ligamentous, osseous, and neural tissue very well (see Chapter 7).164 MRI is noninvasive and does not expose the patient to radiation. Although it has become a widely prescribed imaging test, it is expensive, requires patient cooperation to minimize artifact, and is often not tolerated by claustrophobic patients. Patients with embedded metallic objects such as pacemakers or prosthetic heart valves cannot undergo MRI. Contrast-enhanced CT can accurately evaluate disk pathology163 in these cases. Because cervical intervertebral disk abnormalities occur in asymptomatic patients,20,93,152,157,240 the clinical findings have to be correlated with the imaging findings to accurately diagnose the lesion responsible for the patient’s signs and symptoms.
Electrodiagnostic Evaluation
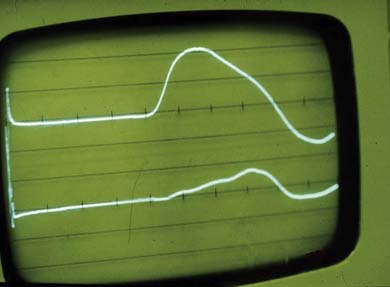
Nerve conduction studies and electromyography can be used to assess the neurophysiologic function of the nerve roots, plexus, and peripheral nerves. Electrodiagnostic examinations, if performed by an appropriately trained physician, can clarify or confirm the suspected diagnosis. Electrodiagnostic examination is also helpful in determining the prognosis of nerve injury. The American Association of Neuromuscular and Electrodiagnostic Medicine guidelines for the electrodiagnostic examination for a radiculopathy include abnormalities in two or more muscles innervated by the same root but different peripheral nerves, provided that normal findings are observed in muscles innervated by adjacent nerve roots.252 At least one corresponding motor and sensory nerve conduction study should be performed in the involved limb to ensure the absence of a concomitant plexus or peripheral process. If abnormalities are found, the correlating contralateral muscle and nerves should be examined to exclude a generalized process such as peripheral neuropathy or motor neuron disease. A screening examination of six upper limb muscles in addition to the cervical paraspinals can identify 94% to 99% of cervical radiculopathies.57 These studies can effectively exclude other diagnoses such as brachial plexus lesions (such as Pancoast tumor or Parsonage-Turner syndrome) and focal peripheral entrapments (such as carpal tunnel syndrome and ulnar entrapment at the elbow or wrist). If the amplitude of the affected muscle’s compound muscle action potential is reduced by less than 50% of that of the contralateral limb (Figure 37-18), functional motor recovery will probably return with conservative care, and studies can be repeated to document neurophysiologic healing (see Chapters 9 through 11).108
Treatment
Physical Medicine and Rehabilitation
The primary objectives of treatment of cervical radiculopathy include the resolution of pain, improvement in myotomal weakness, avoidance of spinal cord complications,64,254 and prevention of recurrence.254 Despite few outcome studies comparing surgical to medical rehabilitation and interventional (conservative) care, accumulated evidence supports the natural resolution of cervical radicular symptoms with conservative care.53,87,199,217 The treatment approach must be molded to the individual patient. A definitive indication for a surgical approach is a progressive neurologic deficit. Otherwise the patient’s necessary level of posttreatment function can help dictate how aggressively to intervene. For example, a relatively sedentary patient might decide to tolerate a low level of discomfort after conservative care. An athlete, on the other hand, might not want to settle for symptoms that are exacerbated by extreme physical activity. The design of the treatment plan has to take into account how the individual functions at home, at work, and in the community.
Modalities
Patient education, activity modification, and relief of pain are the initial treatment steps. The treating physician should explain to the patient the mechanism of how the injury occurred and the most likely treatment outcomes. This explanation should emphasize the importance of proper posture, biomechanics, and the utility of an ergonomic evaluation.254
Thermotherapy is often used to modulate pain and to increase muscle relaxation.134,161 No definitive guideline has been published to date regarding the role of thermal modalities in cervical radiculopathy.191 Cold can be applied for 15 to 30 minutes one to four times a day, and superficial heat can be applied up to 30 minutes two to three times a day. The decision regarding which thermal agent to use is driven by the patient’s perception of which provides the best pain relief.132 Deep heating modalities such as ultrasound should be avoided in the treatment of cervical radiculopathy, because an increased metabolic response and subsequent inflammation can aggravate the nerve root injury.134,191
TENS is helpful in the management of various musculoskeletal and neurogenic disorders (see Chapters 20 through 22). It can be used early in the treatment course of cervical radiculopathy to help modulate pain and enable the patient to engage in other therapeutic modalities. TENS is believed to act via the gate theory. Stimulating large myelinated fibers presumably blocks nociceptive transmission in smaller fibers at the level of the spinothalamic tract neurons.159 Although TENS has been shown to provide some relief of low back pain,229 no studies have been published demonstrating conclusive evidence of its efficacy in cervical radicular pain.
Cervical orthoses function to limit painful range of motion and facilitate patient comfort during the acute injury phase (see Chapter 16).191 Soft cervical collars limit flexion and extension by approximately 26%,109 and are prescribed as kinesthetic reminders of proper cervical positioning.254 The narrower segment should be positioned anteriorly to maintain the neck in the neutral or slightly flexed position (see Figure 37-15).64,199,254 The exceptions to this include patients with a positive L’hermitte’s sign and those with rheumatoid arthritis or atlantoaxial subluxation. The use of a soft collar should be limited to the first week or two of symptoms54,127 to minimize adverse outcomes related to further soft tissue deconditioning.
Cervical traction applies a distractive force across the cervical intervertebral disk space. It is commonly used by patients with cervical radiculopathy, despite a lack of proven efficacy.64,254 It is presumed to work via the decompression of cervical soft tissues and intervertebral disks.47,236 Superficial heat, massage, and/or TENS therapy can be performed before and during traction to relieve pain and to help relax the muscles.46,47 A force of 25 lb is required to distract the midcervical segments when applied for 25 minutes at an angle of pull of 24 degrees.46 Cervical traction can be executed with an intermittent heavyweight or a continuous lightweight regimen in the therapy gym or home setting.47 Traction is contraindicated in patients with myelopathy, positive L’hermitte’s sign, rheumatoid arthritis, or atlantoaxial subluxation (see Chapter 20).47






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


