Collagenase Injection for Dupuytren Contracture
Lawrence C. Hurst
Aaron Insel
Justin B. Mirza
INDICATIONS
Collagenase Clostridium histolyticum (CCH) (Xiaflex), Auxilium Pharmaceuticals, Inc., Chesterbrook, PA, was U.S. FDA approved for the treatment of adult patients with Dupuytren contracture and a palpable cord in 2010. It is an office-based, minimally invasive, nonsurgical treatment. The indications for injectable collagenase are the same as the indications for surgical treatment of Dupuytren contractures including
Metacarpophalangeal (MP) joint contractures of greater than 20 degrees
A progressive proximal interphalangeal (PIP) contracture of greater than 20 degrees
A positive tabletop test
Contracture(s) affecting a patient’s hand function and ability to perform desired tasks
First web and/or thumb contractures that interfere with pinch or grasp
CONTRAINDICATIONS
Injectable CCH is contraindicated in patients with a history of severe allergic reaction to Xiaflex or to collagenase used in any other therapeutic application. Caution should be taken in patients with coagulation disorders or those taking anticoagulant medications other than low-dose aspirin within 7 days prior to receiving a CCH injection, as CCH may exacerbate the expected ecchymosis response after injection. Caution should also be exercised in a finger that has already had surgical fasciectomy, fasciotomy, trigger finger release, or other surgery. Previous surgery can lead to abnormal scar, adhesions, A2 pulley rupture, and occasional skin loss especially at the base of the fifth finger. These postoperative abnormalities can increase the risk for skin tears and tendon injuries during recurrent Dupuytren cord injection. Despite this caution, CCH can be used for Dupuytren cords that develop after surgery when physical examination shows the skin is in good condition and the flexor tendon sheath is intact.
PREPARATION
Initial patient evaluation consists of a thorough history and physical exam including accurate measurements of MP and PIP contractures with a goniometer and recording the tabletop test result. When indicated by clinical exam, plain radiographs of the hand should also be obtained to evaluate possible arthritic joints. After a patient is assessed and deemed an appropriate candidate for injectable CCH, the procedure, risks, potential benefits, and alternatives should be discussed. Next, appropriate paperwork is submitted
to verify insurance benefits. The co-pay responsibilities are also reviewed with the patient. The drug will be either shipped by a specialty pharmacy to the physician’s office or ordered by the office directly from the manufacturer, depending on the patient’s insurance coverage.
to verify insurance benefits. The co-pay responsibilities are also reviewed with the patient. The drug will be either shipped by a specialty pharmacy to the physician’s office or ordered by the office directly from the manufacturer, depending on the patient’s insurance coverage.
Vials of CCH powder and diluent should be stored in a refrigerator at 2°C to 8°C (36°F to 46°F) in the upright position. CCH can be maintained in cold storage until the expiration date. The CCH vials should be allowed to come to room temperature 15 minutes before mixing. If the CCH should accidentally stay at room temperature for more than 60 minutes, both the CCH powder and diluent should be discarded.
The patient should be briefly re-examined prior to the injection by rechecking baseline neurovascular status, tendon status, and cord patterns. A patient with previous surgery should be assessed for possible bowstringing of the flexor tendons that can simulate a Dupuytren cord. Finally, the pathologic cord and the targets for injection are carefully visualized and palpated.
MIXING PROCEDURE
The mixing procedure requires two 1-cc hubless syringes with ½-inch fixed 27-gauge needle and 0.01-mL graduations. This syringe avoids drug remaining in the needle hub while the fixed needle avoids detachment of the needle during injection into the dense Dupuytren cord material. Remove the caps from both vials and swab with alcohol. Insert one needle into the diluent vial and withdraw the appropriate amount of sterile diluent, 0.39 mL for an MP joint and 0.31 mL for a PIP joint (Table 28-1). The diluent is mildly viscous. Next, the diluent is injected into the vial with lyophilized CCH powder. Discard the diluent vial and syringe used for reconstitution. Next, gently swirl the vial until the powder is completely dissolved, which should only take a few seconds. Avoid any vigorous shaking as this could denature the enzyme. Next, orient the vial such that the rubber stopper’s longitudinal cutout is clearly visible and insert a new 1-mL syringe with fixed 27-g needle into this cutout area within the vial (Fig. 28-1). Withdraw the appropriate amount of reconstituted CCH depending on the joint contracture being treated, 0.25 mL for MP and 0.20 mL for PIP. Either volume will provide an actual dose of 0.58 mg of CCH. Once in solution, the drug is quite vicious. If an air bubble occurs while drawing up the diluent, the bubble can be removed by reinjecting the diluent into the bottle and slowly reaspirating the diluent into the syringe.
TABLE 28-1 Volumes of Diluent and Reconstituted Collagenase for Injection | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
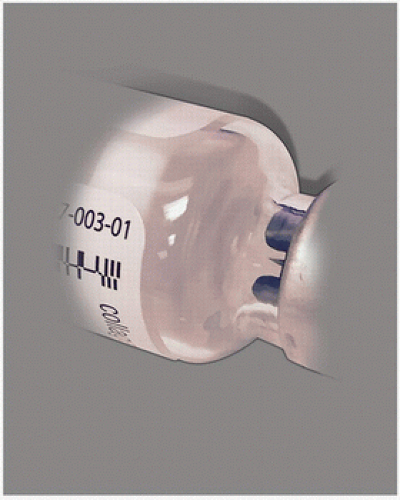 FIGURE 28-1 When drawing up the therapeutic CCH dose, proper position of the 27-gauge needle in the vial is just inside the rubber stopper. This position provides access to all the diluted drug and avoids air bubbles in the syringe. |
It has now been shown that two doses (0.58 mg + 0.58 mg) can be given simultaneously for multiple joints or separate digits (4,18). Therefore, the “off-label” use of some of the residual drug from a single vial can be added to the 0.58 mg dose when injecting especially thick cords or complex cord combinations such as a large “Y” cord (central cord plus a natatory cord).
INJECTION PROCEDURE
Inject the reconstituted CCH at a location where there is maximum separation of cords from underlying flexor tendons, that is, where cord is “bowstrung” away from the flexor tendon sheath (Fig. 28-2).
It is important to hold the cord under tension throughout the injection process to aid in accurate placement of the collagenase within the cord (Fig. 28-3A). Ideally, tension is provided by an assistant or nurse so the surgeon has both hands available to safely manipulate the injecting syringe (Fig. 28-3).
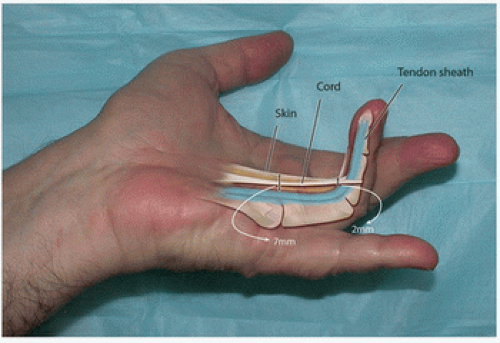 FIGURE 28-2 The Dupuytren cord and its relationship to the flexor tendon sheath is shown. Note cord “bowstrings” away from the flexor sheath, particularly in the palm. Note, the ultrasound verified distances between the skin and flexor sheath in the palm and finger. Skin to sheath distance is 7 mm in palm and 2 to 4 mm at PIP joint. |
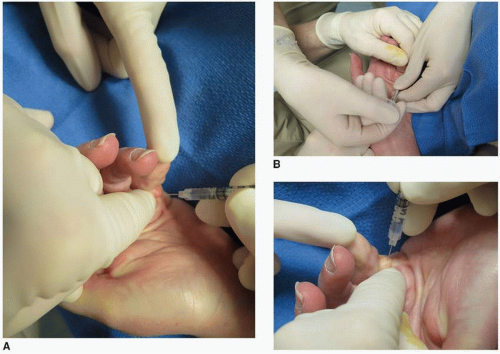 FIGURE 28-3 A: Proper positioning of the digit by an assistant during injection of CCH. Surgeon placing first drug aliquot in distal central cord but avoids area near PIP joint flexion skin crease. B: Surgeon pushes plunger while stabilizing syringe barrel with opposite hand. Assistant maintains tension on cord. |
Related posts:
 Operative Fixation of Juxta-Articular, Intracapsular, and Diaphyseal Fractures of the Phalanges and Interphalangeal Joints
Operative Strategies for Basilar Thumb Fractures: Rolando’s and Bennett’s Fractures
Zone 1 Flexor Tendon Injuries
Zone II Flexor Tendon Repair
Motor Nerve Transfers for Radial and Ulnar Nerve Injuries
Decision Making and Performance of Digital Ray Amputation
Operative Fixation of Juxta-Articular, Intracapsular, and Diaphyseal Fractures of the Phalanges and Interphalangeal Joints
Operative Strategies for Basilar Thumb Fractures: Rolando’s and Bennett’s Fractures
Zone 1 Flexor Tendon Injuries
Zone II Flexor Tendon Repair
Motor Nerve Transfers for Radial and Ulnar Nerve Injuries
Decision Making and Performance of Digital Ray Amputation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


