INTRODUCTION
Thumb hypoplasia encompasses a wide spectrum of presentations from thumbs that have minimal hypoplasia to thumbs with complete absence. As thumb hypoplasia is part of the continuum of radial deficiency, it is important to perform a workup of associated entities such as thrombocytopenia absent radius (TAR) syndrome, Fanconi anemia (FA), Holt-Oram syndrome, CHARGE syndrome, and VACTERL association (
1) (
Table 33-1). Due to the wide variation in presentation, a variety of treatment options exist based on the classification of the hypoplastic thumb.
Classification of thumb hypoplasia is most commonly applied utilizing the Blauth classification, which is an expansion of Muller’s original classification (
2,
3). The focus of this chapter will be on the diagnosis and treatment of type II and IIIa thumbs, which are the thumbs that can undergo reconstruction as opposed to pollicization (
Table 33-2). Both type II and type IIIa thumbs are hypoplastic with decreased size compared to a “normal” thumb. Additionally, both types have absence of the intrinsic thumb musculature (
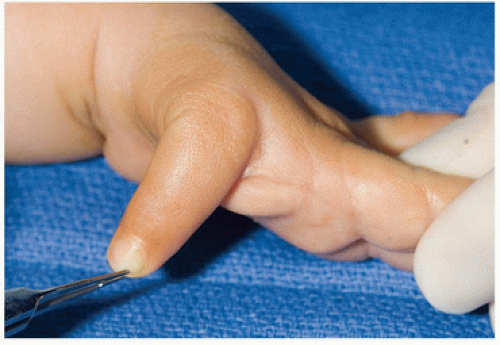
Fig. 33-1), a narrow thumb-index web space (
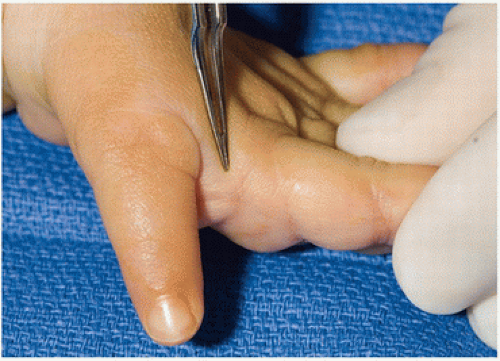
Fig. 33-2), and ulnar collateral ligament (UCL) deficiency (
Fig. 33-3). The UCL deficiency may be due to a deficiency of the ligament or secondary to an anomalous connection between the flexor pollicis longus (FPL) and extensor pollicis longus (EPL) tendons, known as a pollex abductus (
4,
5,
6). The presence of a pollex abductus leads to UCL insufficiency by attenuating the UCL over time and preventing active interphalangeal (IP) joint motion. Release of the pollex abductus must be performed during UCL reconstruction, when present.
In addition to the aforementioned features, type IIIa thumbs have extrinsic muscle and tendon abnormalities (
7). Additionally, skeletal deficiency may be present, but the thumb carpometacarpal (CMC) joint remains stable. The extrinsic tendon abnormalities may involve the extensor side, with an absent or hypolastic EPL or extensor pollicis brevis, or the flexor side, with an absent or hypoplastic FPL. These deficiencies are manifested as decreased or absent thumb IP joint motion. Additional anomalies may include tendon adhesions, tendon duplications, abnormal tendon or muscle routes, abnormal insertions, absent tendons, or underdeveloped pulleys (
8,
9,
10,
11,
12).
Treatment of type II and IIIa thumbs is aimed at correcting the thumb hypoplasia utilizing a combination of procedures to address the functional limitations. The stability provided by the ligamentous structures of the thumb, in particular the UCL, is imperative to permitting the use of the thumb as a stable post during pinch and grasp. Reconstruction of the UCL will provide the necessary
stability to perform these functions. However, the presence of bidirectional or global instability may be best treated by reconstruction of the radial and UCL or preferably with a chondrodesis of the metacarpophalangeal (MCP) joint to achieve firm stability and provide a stable fulcrum. Opposition of the thumb is critical during grasp activities and can be achieved by performance of an opponensplasty. Lastly, deepening of the thumb-index web space is important to permit acquisition of large objects during grasp (
Fig. 33-4). This involves rearrangement of the skin as well as deeper soft-tissue release.
During reconstruction of type IIIa hypoplastic thumbs, additional procedures may be necessary such as the division of anomalous tendon interconnections, rerouting of extrinsic tendons, or pulley reconstruction. Tendon transfers including a ring finger flexor digitorum superficialis (FDS) to FPL or extensor indicis proprius (EIP) to EPL may help to restore the function of thumb IP joint flexion and extension, respectively (
13). These procedures are complicated by the lack of pulleys and deficiency of the entire flexor sheath. Hence, we focus our surgical reconstruction of the intrinsic abnormalities and often ignore the extrinsic deficiencies.


 Operative Fixation of Juxta-Articular, Intracapsular, and Diaphyseal Fractures of the Phalanges and Interphalangeal Joints
Operative Fixation of Juxta-Articular, Intracapsular, and Diaphyseal Fractures of the Phalanges and Interphalangeal Joints



