Closed Reduction and Percutaneous Pinning
Louis W. Catalano III
O. Alton Barron
Indications
Extra- and intra-articular fractures
AO (Arbeitsgemeinschaft für Osteosynthesefragen, the Association for the Study of Questions of Surgical Fracture Fixation) type A2, A3, C1, and C2 fractures
Contraindications
AO type B (shear) fractures
Severe metaphyseal or intra-articular comminution (AO C3 fractures)
Poor bone stock (moderate to severe osteoporosis)
Preoperative Preparation
Initial closed reduction and sugar tong splint application is attempted in all fractures. If the reduction is satisfactory, continue the splint and repeat the radiographs weekly. If closed reduction is unsatisfactory or if the reduction is lost, surgery is recommended.
The authors rarely order preoperative computed tomography (CT) scans. CT scans are obtained if an unusual fracture pattern or notable articular incongruity is present. A preoperative magnetic resonance image (MRI) is obtained if scapholunate joint widening is noted on the pre- or post-reduction radiographs to evaluate a possible scapholunate joint ligament injury.
Obtain a thorough history and perform a physical examination to determine if any signs or symptoms of acute carpal tunnel syndrome exist. If so, perform a concomitant carpal tunnel release.
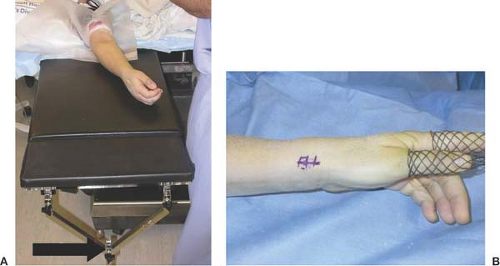 Figure 3-1 A: Photograph of the radiolucent hand table with a traction outrigger at the end of the table. (arrow). B: The finger traps allow for 4.5 kg (10 lb) of longitudinal traction to be applied. |
Technique for Typical Fractures without Excessive Comminution
Use a longitudinal traction table to apply 2.25 to 4.5 kg (5–10 lb) of traction across the fracture to restore radial length (Fig. 3-1A, B).
Perform closed reduction by applying volarly directed pressure on the dorsal aspect of the distal radius fracture fragment (Fig. 3-2A, B). This should restore volar tilt. Occasionally, a 0.062 Kirschner wire (K-wire) will be placed dorsal to volar through the fracture site to use as a lever to create volar tilt.
Use ulnarly directed force on the fracture fragment to reduce any radial translation at the fracture site.

Figure 3-2 A, B: Clinical photograph and radiograph of surgeon applying volar pressure on the dorsal aspect of the distal radius, thereby restoring volar tilt.
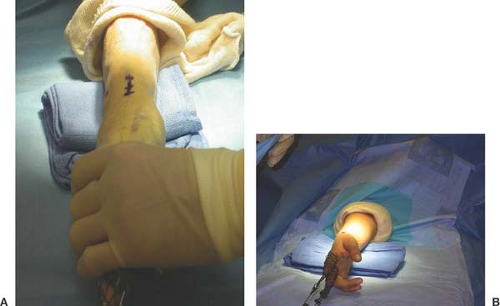
Figure 3-3 Clinical photograph demonstrating how the bump along with the longitudinal traction serves to deviate the wrist ulnarly.
Place two folded towels beneath the wrist. As longitudinal traction is continued, the bump serves to ulnarly deviate and flex the wrist (Fig. 3-3).
Use an image intensifier to verify fracture reduction (Fig. 3-4A, B).
Make a 2-cm incision starting at the tip of the radial styloid and extended distally (Fig. 3-5).
Identify and protect the superficial radial nerve and first dorsal compartment tendons are (Fig. 3-6).
Confirm maintenance of the reduction as an assistant inserts the K-wires.
Using a tissue protector, insert a 0.062 K-wire obliquely from the radial styloid tip aimed proximal and ulnar to engage the ulnar cortex of the radius proximal to the fracture site (Fig. 3-7).
Use intraoperative fluoroscopy to verify satisfactory fracture and K-wire position (Fig. 3-8).
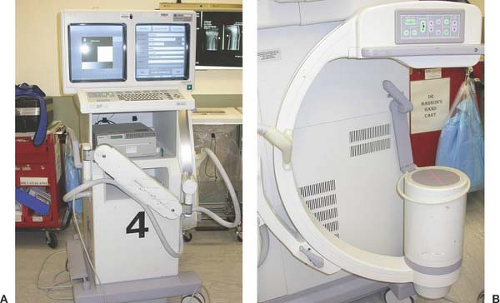
Figure 3-4 A, B: The portable image intensifier allows the surgeon to get good quality intraoperative radiographs with limited radiation exposure.

Figure 3-5 A: A 2 to 3 cm incision is made starting at the radial styloid and extended distally.

Figure 3-6 The large arrow demonstrates the tendons within the first dorsal compartment. The small arrow is pointing to the superficial radial nerve.

Figure 3-7 The tissue protector protects the superficial radial nerve during Kirschner wire insertion.

Figure 3-8 Fluoroscopic image after insertion of the first Kirschner wire demonstrating satisfactory position of the Kirschner wire.

Figure 3-9 A second intraoperative image demonstrating satisfactory position of both Kirschner wires.
Insert a second and (occasionally a third) 0.062 K-wire adjacent to the first K-wire at a slightly different obliquity both in the coronal and sagittal planes into the ulnar cortex proximal to the fracture site.Related posts:
 Arthroscopic-Assisted Limited Open Reduction
Arthroscopic-Assisted Limited Open Reduction
 Distal Radius Osteotomy
Distal Radius Osteotomy
 Scapholunate Advanced Collapse (SLAC) Reconstruction: Four-Corner Arthrodesis with Headless Screws
Scapholunate Advanced Collapse (SLAC) Reconstruction: Four-Corner Arthrodesis with Headless Screws
 Partial Excision of the Triangular Fibrocartilage Complex
Partial Excision of the Triangular Fibrocartilage Complex
 Arthrodesis of the Rheumatoid Wrist
Arthrodesis of the Rheumatoid Wrist
 Release of the First Dorsal Compartment
Release of the First Dorsal Compartment

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


