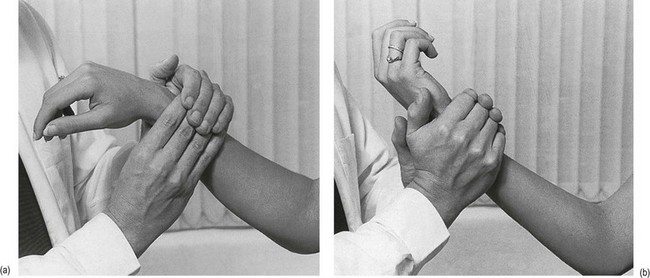
20 • The tendons that control the wrist • The trapezium–first metacarpal joint • The tendons that control the thumb • The tendons that control the fingers • What is the problem? The patient describes the symptoms that are experienced in the wrist, thumb, hand or fingers. They are variable and may include pain, paraesthesia, numbness and weakness. • How did it start? Was there an injury? Especially when a capsular pattern is found during the examination, the possibility of a fracture must be considered. • Or did it start after particular exertion? Most ligamentous, muscular or tendinous lesions result from overuse. The symptoms may have started spontaneously, as usually happens in arthrotic or arthritic disorders. • How has the problem developed? Because of the distal localization of the lesion, its evolution can only be judged in terms of the intensity of the symptoms, or by their appearance or disappearance, but not by reference of the symptoms. The typical articular deformities of arthrotic or arthritic changes in the joints are well known. The wrist, thumb and hand are examined using 21 tests (Box 20.1). The patient holds the elbow in 90° flexion. The examiner grasps the patient’s forearm just proximally to the wrist with both hands. The heel of the contralateral hand is placed on the palmar aspect of the ulna, the fingers of the other hand at the dorsal aspect of the radius. Pronation is performed by a simultaneous movement of both hands (Fig. 20.1a). The normal end-feel of flexion and extension is capsular (elastic). If these movements are positive, the examiner must be able to tell whether the condition is of the capsular or the non-capsular type (see Ch. 23).
Clinical examination of the wrist, thumb and hand

Referred pain
History
Inspection
Functional examination

The distal radioulnar joint
Passive pronation
The wrist
Passive movements (Fig. 20.2)
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Clinical examination of the wrist, thumb and hand