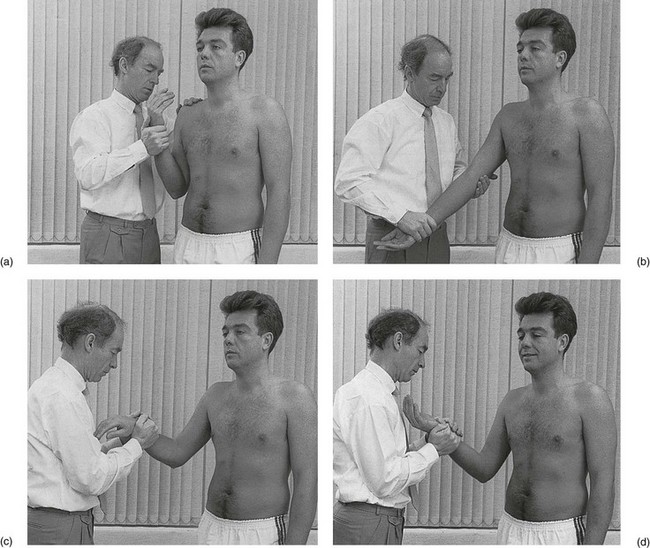
16 The history is not very important in elbow problems but some questions should be asked. • Where is the pain? The location of the pain is usually closely related to the site of the lesion. When the patient indicates exactly where the symptoms are felt, all causes that cannot produce pain in that area are automatically excluded. • How did it all start? Did the symptoms start spontaneously or has there been any trauma; if so, what type? If the onset was spontaneous, did it begin suddenly or gradually, or as the result of a particular activity? • What was the evolution? Was there any change in the location, intensity or frequency of the painful episodes? Did the pain spread and, if so, where to? This may indicate the dermatome and, in consequence, the segment in which the lesion must be sought. • Is there any functional loss? • Has the elbow ever been swollen? If the swelling came on after trauma, how soon did it appear? Immediate general effusion is probably the result of a haemarthrosis; gradually increasing swelling usually indicates the presence of synovial fluid. Spontaneous swelling may be the result of an impacted loose body or a rheumatoid condition. Localized swelling may occur in bursitis or in some exceptional cases of tennis elbow. • What influences the pain? Is the pain constantly present, or does it come on during or after either general or specific activity? In an arthrotic or arthritic joint the maintenance of a particular posture at the extreme of the possible range may become very painful. Release from this position is usually very uncomfortable. ‘Twinges’ when picking up objects (e.g. a telephone or a coffee pot) with an outstretched elbow is a well-known symptom in tennis elbow. • Are any other joints involved? In rheumatoid-type conditions other joints may be affected. The examination consists of 10 tests: four passive movements and six resisted movements. The passive movements (Fig. 16.1) are used to examine the inert structures: the joint, the capsule, the capsular ligaments and the bursae. It is also clear that, by passively testing the elbow, one also indirectly stretches or pinches muscular and tendinous structures. The range of movement is ascertained and the end-feel noted.
Clinical examination of the elbow

History
Functional examination

Passive movements
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Clinical examination of the elbow