Chapter 5 Clinical correlations in sports
Clinical correlations: specific biomechanical changes
Clinical correlations: specific sports
A ‘natural’ process of elimination
Effect of malalignment on the validity of research in sports
2. engage in sports that involve repeated:
Malalignment itself may occur secondary to:
1. insults of this type; in particular, strains, falls and fractures, also
2. repeated asymmetrical throws and torsional stresses (e.g. lacrosse, baseball, tennis).
1. whether failure to advance in some sports:
2. the effect of malalignment on the validity of research that involves investigation of biomechanical aspects of certain sports and treatment techniques.
Clinical correlations: specific biomechanical changes
Vertebral rotational displacement
In the thoracic region, stress resulting from a vertebral displacement is also transmitted through the costovertebral and costotransverse joints to the ribs, and anteriorly to the sternocostal and costochondral junctions (Figs 2.94, 3.15, 3.16). Further rotation into the direction of the displacement is restricted, affecting the overall movement of the spine and predisposing to injury.
The term ‘vertebral rotational displacement’ refers to excessive rotation of one or more vertebrae relative to those immediately above and below (see Ch. 2), which can result in increased stresses and strains on soft tissue structures, facet joints and discs at the level(s) involved.
Vertebral levels commonly involved
The general findings on examination at an affected level have been described in Ch. 2. Rotational displacement can affect any vertebra between the occiput and the sacrum but it does involve certain levels of the spine with increased frequency (see Ch. 3). Note is here made of some of these levels.
L4, L5 or both vertebrae
Though these are involved infrequently (affecting some 5% of those with recurrent pelvic malalignment), there are three major problems that can result with rotational displacement at these levels: pain, restriction of range of motion and secondary malalignment of the sacrum and the SI joints (Figs 2.52, 2.96). Instability of the lumbosacral area may be caused by the initial injury or develop subsequently with the stress arising from recurring vertebral rotational displacement.
Pain
1. increased tension on soft tissue structures
Clockwise rotation of L5, for example, increases tension in the right iliolumbar as well as the supra- and interspinous ligaments, also multifidi and rotatores muscles, primarily from the L3 to S1 level (Figs 2.29, 2.52B, 3.68). It compresses the left and separates the right L5–S1 facet surfaces. Distraction or entrapment of the facet joint capsule, ligaments and the nerve fibres supplying these joints can account for localized pain and referred symptoms to the ipsilateral buttock and lower extremity as far down as the ankle (McCall et al. 1979; Mooney & Robertson 1976; Travell & Simons 1992).
Restriction of range of motion
The ‘FRS’ and ‘ERS’ patterns result in a restriction of further movement into the directions indicated. L1–L4, for example, would normally rotate into a convexity; therefore, rotation would be counterclockwise into a left (Figs 2.42, 4.6, 4.26, 4.33) and clockwise into a right convexity (Fig. 2.96A). Superimposing a clockwise rotational displacement of L4 on a pre-existing right convexity will accentuate the already existing forward flexion (or extension), rotation and right side-flexion, limiting any further movement of L4 into all of these directions. Counterclockwise displacement of L4 would limit further movement into the opposite directions (Fig. 2.96B).
1. Assuming that the lumbar spine is forward flexed and L1-L4 have rotated clockwise into a right lumbar convexity (Fig. 2.96A):
2. if L4 now rotated to the left, its range of rotation into the opposite (left) FRS directions may be slightly increased
3. if L4 rotated even further to the right with an excessive force, it could be literally ‘jammed’ into a right FRS position.
Malalignment of the SI joints
A clockwise rotation of L4 or L5 exerts a rotational force on the innominates (anterior on the left and posterior on the right) because the simultaneous rotation of the transverse process – forward on the left, backward on the right – displaces the iliolumbar ligament origins away from their insertions and increases tension in these ligaments on both sides (Fig. 2.52A). There is also the torsional effect on the sacrum transmitted through the compressed left facet joint (Fig. 2.52B) and the L5-S1 disc. Reactive spasm in the adjacent quadratus lumborum and psoas can cause a recurrent ipsilateral ‘upslip’ (Fig. 2.62). Always remember that in the case of recurrent ‘rotational malalignment’ or an ‘upslip’, two common causes to consider (especially when there is excessive pain, usually acute in onset) are:
Thoracolumbar junction: T11, T12 and L1
1. pelvic obliquity and the compensatory scoliosis that creates stress points at the sites of reversal: the lumbosacral, thoracolumbar and cervicothoracic junctions
2. ‘facilitation’ of the left quadratus lumborum muscle; this increase in tension would act directly on the upper origins of this muscle from the L1 transverse process and may help explain the frequently seen L1 left vertebral rotation
3. ‘thoracolumbar syndrome’ (see Ch. 4; Figs 4.20–4.23)
4. rotational stresses on the attaching rib(s) and thoracic diaphragm
A rotational displacement of T11 and/or T12 results in increased stress on their costovertebral and costotransverse articulations. The associated torquing increases the stress on the anterior articulation of the 11th rib at the costochondral junction and its continuation as the costal cartilage. Pain can usually be provoked by applying pressure anywhere along the affected rib(s), and localized by direct pressure on the tender anterior and/or posterior articulation(s). Torsion of the lower ribs can also present as discomfort and even spasm of the attaching diaphragm. Any of these structures may become symptomatic, sometimes presenting as ‘chest’ or ‘abdominal’ pain and leading to extensive investigations to rule out a cardiac, respiratory or gastrointestinal problem (see Ch 4).
The T4 and T5 level
1. reversal of the curvature of the thoracic segment, which helps to ensure that the head ends up in the midline, may start as low as T4 or T5 (Fig. 2.91B)
2. forces normally associated with upper extremity activities intersect at this level; unopposed or unequal forces predispose to displacement of one or both vertebrae through muscle action (e.g. different muscles on opposite sides that can created a torsional component when acting together; unopposed unilateral rhomboid action because of weakness of its partner or a difference in tone, with ‘facilitation’ on one side and ‘inhibition’ on the other):

The associated pain is commonly felt in the interscapular area and/or under one or both scapulae. Pain from these sites can also be referred directly through the thorax to the anterior chest region, simulating angina (see Ch. 4). Other referred pain patterns to the shoulder girdles were discussed in Ch. 2 (Figs 3.12, 4.8). The athlete may localize the discomfort mainly to an area of increased tension and tenderness, or actual localized spasm. These changes may be palpable within the immediately adjacent rhomboid, mid-trapezius and paravertebral musculature (sometimes just on one side), or more laterally (e.g. subscapularis, infraspinatus, teres minor). The abnormal tension may simply reflect an increase in distance between the origin and insertion of these muscles. For example, a right deviation of the T4 spinous process, away from the left scapula, will increase tension in the attaching left rhomboid and mid-trapezius muscles. Alternately, the vertebral rotation may be secondary to an increase in tension with spasm, sprain or other injury affecting right rhomboid, pulling T4 to the right. Pain from T4/T5 can also trigger a reflex contraction of adjacent muscles in an attempt to splint this site. One is usually looking at a combination of factors (see Ch. 3). The area may, however, remain asymptomatic. Just as an imbalance in muscle tension can cause rotation of a vertebra in the interscapular region, specific muscles can be harnessed to rotate that vertebra back in line (see Ch. 7: ‘using rhomboid to effect realignment of T3’; Fig. 2.97).
On examination, pain may be evoked with posterior-to-anterior and/or rotatory pressure to the spinous process of the vertebra, possibly also to the one above and below. There may be discomfort with pressure applied to the soft tissues within the immediate vicinity. As in tests carried out for thoracolumbar syndrome, the findings may suggest an irritation of specific facet joints (Fig. 4.20). Trigger points are common in the muscles and ligaments at these levels and the adjacent posterior shoulder girdle regions. In addition, upper extremity ranges of motion may be restricted if they exert a rotational force on a tight, affected segment of the thoracic spine and provoke pain.
The ‘T3’ or ‘T4’ syndrome
As initially described by Maitland (1977), this refers to a symptom complex caused by the rotation of one or more vertebrae between T2 and T7, with T3 or T4 being most commonly involved. The symptoms are vague and widespread, with a report of pain and paraesthesias in the upper limbs and/or head pain (initially described as a dull aching or pressure feeling in an ‘all-over’ distribution). Symptoms may occur as a result of referral through the autonomic nervous system, originating from the upper thoracic region. In the series of 90 patients with T4 syndrome published by McGuckin in 1986, all had involvement of the upper extremity, either uni- or bilaterally, with a glove-like distribution of paraesthesias: fingers up to the wrist(s), or to the forearm, elbow or an even more proximal level (Fig. 4.9).
Examination and diagnostic techniques
1. non-specifically on side-flexion, back extension alone, and back extension combined with rotation to the right or left
2. more specifically, by applying a translatory rotational (Fig. 4.20A) or direct forces to individual spinous processes (Figs 4.20B, 5.2).
Posteroanterior translation or ‘glide’ in the sagittal plane may be similarly decreased or abolished, making the affected level(s) feel ‘stiff’ and unyielding. These changes are usually most easily appreciated in the region of T12–L1, where the reversal of the lumbar and thoracic curves in the sagittal and coronal planes itself already results in a restriction of joint play, even in the absence of any superimposed rotational displacement of one or both vertebrae (Fig. 3.14C). The levels adjacent to a site of such excessive rotation sometimes also lack ‘give’ and feel stiff; whereas hypermobility may be evident at sites immediately adjacent or some distance away, where the spine is attempting to compensate for this restriction of movement or has been stressed to the point that actual ligament laxity or joint degeneration has occurred.
Rib involvement can be assessed by examination for side-to-side asymmetry and by stressing the anterior and posterior rib attachments, either directly or by selectively springing the individual ribs along their length (Figs 2.93, 2.94). Diagnostic nerve root blocks can be helpful if involvement of posterior root or intercostal nerve fibres is suspected. Selective blocks of the rib articulations – costochondral, costotransverse and costovertebral – may also help to localize the origin of the pain (see Chs 3, 4, 7 and Figs 3.15, 3.16).
Correlation to sports: vertebral rotational displacement
Rotational displacement of a vertebra is most likely to become symptomatic with sports that require repeated flexion, extension, rotation or combined motions of the spine. These include, in particular, weight-lifting, court sports, sports involving a swinging motion (e.g. golf, baseball, lacrosse, ice hockey), rowing sports, canoeing, kayaking, throwing events and martial arts. Whether or not such a displacement actually becomes a problem depends on several factors (Box 5.1).
Box 5.1 Factors that influence whether vertebral rotational displacement becomes a problem
1. Restrictions at the level of the spine affected are superimposed on the restrictions already caused by the normal orientation of the facet joints (thoracic more flat or horizontal, limiting flexion and extension; lumbar aligned more in the sagittal plane, limiting rotation; Fig. 3.9)
2. The degree of rotational displacement determines the degree of:
3. The particular sport places further stresses on the level at which the displacement has occurred. Excessive rotation of a lumbar or thoracic vertebra, for example, does not necessarily pose a problem with repetitive, symmetrical flexion/extension activities such as sculling or using a rowing machine. The deciding factor here would be whether the degree of extension required is such that it causes a further approximation on the side on which the surfaces have already been brought closer together, to the point of actually provoking pain.
4. The athletic activity puts an additional rotational stress through the level(s) affected (e.g. court sports or kayaking); this is especially true for the lumbar segment, where the minimal rotation normally available may already have been reduced to a critical point on one side by the rotational displacement.
Sports requiring rotation of the trunk while sitting
The pelvis is now fixed, rotation again occurring primarily through the thoracic segment and at the thoracolumbar junction. Once no further rotation is possible through these levels, the lumbar spine will start to rotate as one segment. Rotation, however, is limited and quickly results in increased stress on the lumbosacral junction. This athlete is, therefore, more likely to develop symptoms from the mid- (thoracolumbar) and low back (lumbosacral) regions with activities such as kayaking, yet may have no problem with asymmetrical paddling. For example, when canoeing in the kneeling position, the rotational stress can be distributed along the length of the spine, the pelvic region and even partly through the lower extremities (Fig. 5.1).
Limitation of sports performance by the common presentations of malalignment
1. interfering with the desired or required range of motion
2. provoking discomfort or pain
3. causing problems with muscle weakness and fatigue
4. altering weight-bearing, balance and controlled progression (ice skating, dancing/ballet)
5. disturbing symmetry, posture and style (synchronized swimming, competitive weight-lifting).
Appendix 10 notes the changes that can occur and some of the sports affected as a result.
Clinical correlations: specific sports
Specific sports create specific demands, and malalignment can affect the ability to meet these demands, often in a predictable manner. We are sometimes too quick to blame hand and foot preference, muscle tightness or weakness in an attempt to explain why one athlete is unable to change his or her style and repeatedly carries out a manoeuvre in the same way, or why another athlete has suffered a specific injury (especially if it is recurrent). A knowledge of the biomechanical changes and limitations imposed by the malalignment may allow for a more rational explanation. Appendix 11 details the clinical correlations related to some specific sports and Appendix 5 lists those specific to running.
Court, racquet and stick sports
Excessive rotation into a pelvic or thoracic restriction
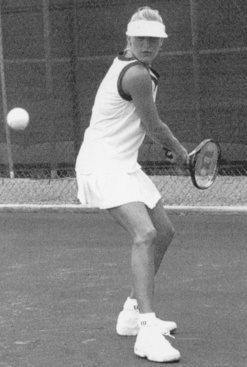
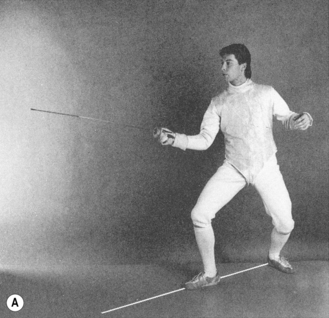
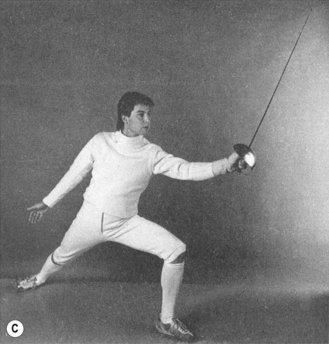
Typical here is the rotation of the trunk required in tennis or golf (see below). Take the example of a ‘right anterior, left posterior’ innominate rotation and a lumbar segment convex to left (Fig. 2.42). When he or she attempts a right backhand with both feet fixed to the ground (Fig. 5.3), the initial left rotation is restricted:
1. through the lumbar segment, by the fact that the vertebrae have already rotated partly to the left, into the convexity (Fig. 2.42)
2. through the pelvic unit around the vertical axis in the transverse plane (Fig. 3.5C)
3. through the legs, especially by a limitation of further left internal, right external rotation, as these are already partially rotated in these directions
1. right pronation and knee valgus angulation
2. left supination and knee varus angulation
Excessive movement into a restricted hip range of motion
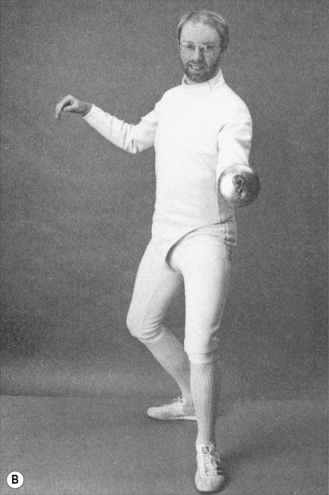
‘Right anterior, left posterior’ innominate rotation results in a limitation of right hip flexion and internal rotation, left hip extension and external rotation ( Figs 3.71–3.75). There is, therefore, an increased risk that a quick forward movement of one leg or backward of the other may exceed the available hip flexion or extension range of motion, respectively. In the example given, there would be an increased risk in a lunge with the right leg leading and the left receding (Fig. 5.10C). Similarly, rotation of the body to the right or left over a planted, relatively ‘fixed’, foot may exceed, respectively, the remaining external or internal rotation available for that extremity, possibly to the point of ‘engaging’ the anatomical barrier and causing injury ( Figs 3.78–3.80, 5.14B,C).
Thoraco-abdominal injuries
Injuries involving rectus abdominis, transversus abdominis and external and internal abdominal oblique muscles have been seen to occur more often in tennis players than in those playing handball and racquetball. Lehmann (1988) may well have been right in attributing these injuries to the increased need for overhead activity in tennis. Malalignment can, however, also increase the chance of suffering a sprain or strain of these ‘inner’ and ‘outer’ core muscles with the sudden rotational, reaching and extension movements characteristic of some of these sports (Figs 5.4A,B,C).
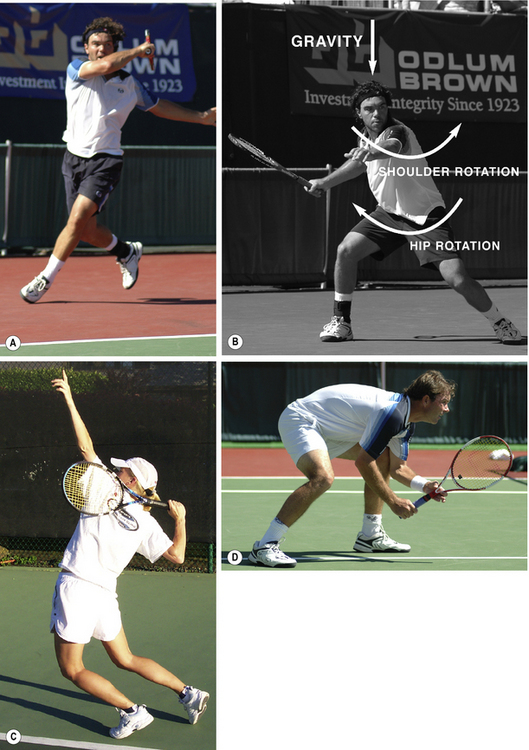
Fig. 5.4 Quick twisting and rotational responses. (A) The player is bearing weight on the left leg only. Note: the left foot is supinated; this athlete would be more liable to suffer an inversion sprain if an ‘upslip’ or ‘rotational malalignment’ were present, with the associated shift in weight-bearing toward left supination and functional weakness in left peroneus longus (see Fig. 3.37). (B) Torsional stresses increase risk of injury to soft tissues and joints in thoracic and lumbar spine regions in particular. (C) Overhead serve, a combination of back hyperextention and trunk rotation, results in torsional and ‘jamming’ (compressive) forces on the back. (D) The forward-flexed posture, common to tennis and a number of other competitive sports, predisposes to malalignment when combined with trunk rotation and side-flexion.
(Courtesy of Petersen & Nittinger 2006.)
Athletes presenting with malalignment sometimes complain of pain in the lateral flank and abdominal region on one or both sides. Problems relating to transversus abdominis or the external or internal obliques can cause pain in these generalized areas, given the overlapping of these muscles and their role as part of the anterior abdominal slings. Tenderness may localize to their origins from the ribs, the main muscle bulk itself or the insertions onto the innominates (Figs 2.31B, 2.32, 2.33).
External abdominal obliques
Most frequently injured, uni- or bilaterally, are the external abdominal obliques (Fig. 2.32) which:
1. originate from the posterolateral aspect of the lower eight ribs and run forward and downward, to
2. insert into the iliac crest and, along with the inferior segment of transversus abdominis and lateral rectus abdominis
3. also insert into the iliohypogastric and ilioinguinal region and onto the lateral aspect of the superior pubic ramus
Tension in the right external muscle is increased by ‘right anterior’ innominate rotation, and by clockwise trunk and counterclockwise pelvic rotation around the vertical axis, also ‘left outflare/right inflare’. Tension increases simultaneously in other abdominal muscles, such as transversus abdominis and rectus abdominis, which are interlinked with the external obliques (Fig. 2.39).
Internal oblique
This muscle originates from the thoracodorsal fascia and anterior iliac crest, inserting into ribs 9-12, through the aponeurosis into the linea alba and to the superior pubic ramus and pectineal line. In the example given above for the effect of ‘right anterior’ rotation on the right external oblique (Fig. 2.32), tension is especially likely to increase in the contralateral (left) internal oblique (Fig. 2.33) if there is a compensatory ‘posterior’ rotation of the left innominate, also with a ‘left outflare’.
Transversus abdominis
Tension will increase in the ipsilateral transversus abdominis (Fig. 2.31). This muscle originates from the lateral inguinal ligament, iliac crest, thoracodorsal fascia and cartilages of the lower ribs, to insert into the linea alba, the superior pubic ramus and the pectineal line.
Rectus abdominis
‘Anterior’ innominate rotation increases tension in the ipsilateral half of rectus abdominis by separating its origin and insertion (Fig. 2.31B). As indicated above, transversus abdominis and the external and internal obliques blend with rectus abdominis and are, therefore, also affected indirectly by tension changes in this muscle.
Tension in all four muscle groups is further increased by reaching and extension movements (e.g. serving in tennis, bowling in cricket, going up for a spike in volleyball). Injury is more likely when rotation, reaching and extension movements occur at a time when these muscles and their tendons are already under increased tension because of pre-existing malalignment (Figs 3.51, 5.4)
Low back pain
Marks et al. (1988) stated that the four strokes used in racquet sports – forehand and backhand ground strokes, the overhead serve and the volley – all put the back at risk. The overhead serve in tennis, for example, is a combined action of rotation and hyperextension of the back (Fig. 5.4B). Rotation occurs through the lower extremities, pelvis and primarily thoracic segment of the spine. Any malalignment-related restriction of movement increases the stress on sites that are already attempting to compensate.
1. restriction of further internal rotation of the left leg and
2. the associated restriction of pelvic rotation around the vertical axis in the transverse plane to that side, especially when both feet are on the ground (Fig. 3.5C).
Pelvic restriction can only increase the stress on the thoracic spine, whose ability to rotate to one side or the other may be further decreased by the rotational displacement of any individual thoracic vertebrae (Fig. 3.49B). It should be remembered that thoracolumbar dysfunction, rather than causing mid-back pain, may be felt as low back pain and also as lateral hip/buttock pain (e.g. as in the ‘thoracolumbar syndrome’ with cutaneous nerve involvement; Fig. 4.23A,B).
Shoulder injuries
Malalignment impairs both shoulder stability and ranges of motion (Fig. 3.17), partly as a result of the:
Those with an ‘upslip’ or one of the ‘more common’ rotational patterns typically show an increase in right external, left internal rotation of the gleno-humeral joint (Fig. 3.17A).
1. the increased external rotation puts these anterior tissues under even more strain, at the risk of stretching and eventual anterior gleno-humeral joint laxity (Fig. 4.7)
2. a forceful swing-through is more likely to come to an abrupt halt by the limitation of internal rotation on the right side if he or she tries to go through the full ROM (Fig. 3.17A)
3. to avoid stressing these anterior tissues, especially if there is already some discomfort, the player may avoid using the extra external rotation available on the right side and instead compensate by increasing rotation and extension of the spine to ‘wind-up’ for the throw, at the risk of precipitating or aggravating back pain (Fig. 3.18).
Groin strain
1. One tends to occur on clay surfaces and involves the leading foot sliding outward. A loss of traction can result in the slide ending up as a split, in which case the adductors, and less often the iliopsoas, can be strained or the lesser trochanter avulsed (Figs 3.50, 5.21)
2. The other mechanism occurs by ‘posting’ the leading foot outward on a surface where the footing is secure, such as a synthetic court. In other words, lateral movement is abruptly stopped. Here ‘the efforts of the adductors and hip flexors are opposed by lateral momentum, and contraction results in muscle tearing rather than the anticipated deceleration’.
The majority of those with the ‘right anterior, left posterior’ rotational pattern present with a restriction of both left hip adduction and abduction range (see also Ch. 6). Tension is typically increased in:
1. the left hip abductors and tensor fascia lata/iliotibial band (TFL/ITB) complex, through ‘facilitation’ (Figs 3.41, 3.44)
2. the iliacus component of iliopsoas (Figs 2.46B,C, 2.59, 3.42, 4.2B), especially when ‘posterior’ innominate rotation is present (which it is more often on the left side; see Ch. 2)
3. iliopsoas as a unit, sometimes unilaterally in an attempt to stabilize an SI joint or decrease pain
4. psoas, as a result of ‘facilitation’ linked to T12, L1 or L2 vertebral rotational displacement.
The combined effect of these restrictions predisposes to injury of the hip adductors, as well as pectineus and the individual components of iliopsoas (Figs 2.62, 4.2. 4.14), with either a lateral ‘slide’ or ‘posting’. Forced adduction can cause pain by compressing these same structures, while putting a tight gluteal/TFL/ITB complex at risk of sprain or strain (Figs 3.41, 3.44Aiii, 5.17).
Reference should also be made at this point to the occurrence of a painful hemipubic bone in court sports as a result of irritation of the anterior cutaneous branches in association with T12/L1 rotational displacement and the ‘thoracolumbar syndrome’ (Fig. 4.23A2,B2; Appendix 9). These branches are vulnerable especially in those playing tennis or soccer (Maigne 1995). Certainly, repeated trunk hyperextension and reaching manoeuvres (e.g. serving), as well as excessive or repetitive hip extension stressing the back, will put the anterior branches under stretch while simultaneously narrowing the intervertebral foraminal outlets as the player leans backward.
Knee injury
Typical alterations of knee biomechanics relating to malalignment, and predisposing to acute injury or accelerated wear and tear, have been discussed above under ‘Excessive rotation into a pelvic or thoracic restriction’ and Ch. 3 (Figs 3.37, 3.81, 3.82).
Ankle sprains
The ‘more common’ rotational patterns and an ‘upslip’ predispose to various types of ankle sprain (Box 5.2 and see Ch. 3).
Box 5.2 Malalignment predisposes to ankle sprains
In someone with an ‘upslip’ or one of the ‘more common’ patterns of ‘rotational malalignment’:
1. left ankle inversion sprains: caused by the tendency to supination and lateral weight-bearing, weakness of the peroneal muscles and pre-positioning by internal rotation of the left lower extremity
2. right ankle inversion sprains: occur less frequently and are probably attributable in some cases to the increase in right varus angulation observed when non-weight-bearing (Fig. 3.26); as the lateral aspect of the right foot hits the ground at this more acute angle, there is a momentary instability of the foot that, literally, can cause it to ‘fall outward’ (instead of rolling into eversion and forward into pronation, as would be usual)
3. right ankle eversion sprains: caused by the tendency to pronation and medial weight-bearing, weakness of the ankle invertors, and pre-positioning by external rotation of the right lower extremity
Collision with a fixture or opponent
As a result of a collision, parts of the body may be involuntarily rotated into one of the restrictions of range of motion imposed by the malalignment, ‘jamming’ a facet or SI joint or actually exceeding the anatomical barrier earlier to the point of causing soft tissue and joint injury (Fig. 2.51B).
Recurrence or aggravation of malalignment
The activities are already asymmetrical, with rotational components, and often also involve repeatedly shifting weight-bearing or jumping from one leg onto the other. Carrying out manoeuvres in a flexed position increases the risk of imbalance (Figs 5.3, 5.4D). Going out of alignment only augments all these asymmetries and any imbalances. Because of the competitive element of a game, movements often occur almost reflexly as the athlete throws all caution to the wind, something which can only add to the risk of sustaining an injury or causing the recurrence or aggravation of an existing malalignment problem.
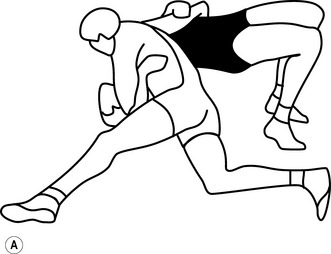
Curling
The curler delivering the ‘rock’ gathers enough momentum to slide about ten meters from the ‘near hack’ line at the back to finally release the rock at the ‘near hog’ line. The position assumed for the slide is similar to a ‘lunge’ (Fig.7.18B). Throwing with the right arm, he or she:
1. weight-bears and slides on the left foot, with the hip and knee fully flexed
2. trails the right leg, with the hip in partial extension and the leg sliding along the top of the ice
3. leans the trunk forward some 20 to 30 degrees but keeps the head level, eyes focused on the target ahead
Basically, the player is in a ‘left leg forward’ lunge position. Assuming the presence of a:
1. ‘right anterior, left posterior’ innominate rotation
2. ‘left anterior, right posterior’ rotation
Malalignment is more likely to precipitate problems on account of:
1. increasing stresses on sites that are already vulnerable because of the posture the player has to assume; namely, the lumbosacral and cervicothoracic junctions
2. repetitive torsion through these same sites on delivery of the rock, with the thorax having to counter any rotational movement of the pelvis.
Cycling






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


