CHAPTER 50 Cervical Myelopathy
Cervical myelopathy implies spinal cord dysfunction in the cervical spine. The etiologies are numerous and these are divided into extrinsic and intrinsic neurogenic conditions (Table. 50.1). Extrinsic neurogenic conditions entail spinal cord compression. Structural abnormalities surrounding the spinal cord contribute to encroachment on the available space in the spinal canal, resulting in spinal cord compression. The spinal cord compression entities are some of the most common conditions in myelopathic patients older than 55 years of age, because these abnormalities are generally due to degeneration of the cervical spine. Intrinsic neurogenic conditions are based on the primary pathology in the spinal cord. These intrinsic pathologies are important as differential diagnoses of compressive myelopathy. This chapter reviews the pathology, diagnosis, and differential diagnosis of compressive myelopathy in the cervical spine.
Table 50.1 The Causes of Cervical Myelopathy
| EXTRINSIC NEURAL CONDITIONS | |
| INTRINSIC NEURAL CONDITIONS | |
PATHOLOGY OF COMPRESSIVE MYELOPATHY IN THE CERVICAL SPINE
Causes of spinal cord compression
Various pathologies have the potential for encroachment in the spinal canal.1–4 Although these conditions do not always result in compressive myelopathy, there is a risk of spinal cord involvement.
Cervical spondylosis
Cervical spondylotic myelopathy (CSM) (Fig. 50.1) is the most common cause of spinal cord dysfunction in patients with compressive myelopathy. Cervical spondylosis initially occurs due to degeneration of the intervertebral disc. Disc degeneration increases mechanical stress at the endplate and this condition results in subperiosteal bone formation. By such a mechanism, osteophytes develop at the upper or lower edge of the vertebral body. Osteophytes at the posterior margin of the vertebral body, which are also called ‘posterior bony spurs,’ have the potential to encroach on the spinal cord. These spondylotic changes are often observed at many levels in the cervical spine. However, the presence of cervical spondylosis alone does not usually lead to myelopathy. The pathology of cervical myelopathy is multifactorial. It is important to consider the context of static and dynamic mechanical factors as well as ischemic factors.5,6

Static mechanical factors
The size of the spinal canal plays an important role in the development of cervical myelopathy.7,8 Spinal canal size is the distance between the posterior margin of the vertebral body and the anterior edge of the spinous process (Fig. 50.2). The normal canal diameter from C3 to C7 is 17–18 mm in Caucasian and 15–17 mm in Japanese.9,10 The canal size in patients with cervical myelopathy is smaller than in those without it (Fig. 50.3).10 It is believed that a sagittal diameter of 12 mm5,6,11 (or 13 mm in some reports4,12,13) or less is a critical factor in the development of cervical spondylotic myelopathy.
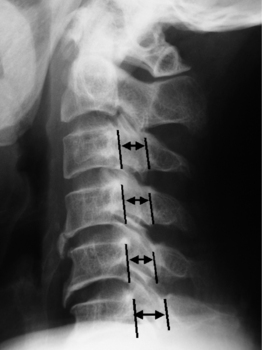
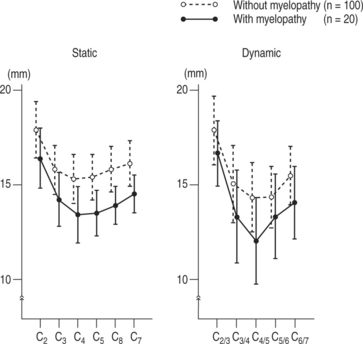
Fig. 50.3 The comparison of the canal size between patients with cervical myelopathy and those without it.
(Hayashi H, Okada K, Hamada M, et al. Etiologic factors of myelopathy. A radiographic evaluation of the aging changes in the cervical spine. Clin Othop 1987; 214:200–209 with permission.)
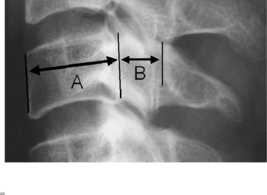
The Pavlov ratio is also used in the judgment of cervical spinal stenosis.14 This is the ratio of the anteroposterior (AP) diameter of the spinal canal to the anteroposterior diameter of the vertebral body at the same level as measured on a lateral radiograph (Fig. 50.4). The merit of this measurement is that the ratio is not affected by variations in radiologic magnification. A normal ratio is 1.0 and a ratio of less than 0.82 indicates cervical spinal stenosis. The Torg ratio is the same as the Pavlov ratio. Torg stated that a ratio of less than 0.8 indicates cervical stenosis.15
Dynamic mechanical factors
In cervical spondylosis, movement of the cervical spine could have an impact on spinal cord compression. During extension of the cervical spine, the ligamentum flavum buckles and it narrows the spinal canal. The spinal cord is compressed between the posterior margin of one vertebral body and the lamina or ligamentum flavum of the next caudal level. In flexion, spinal cord compression occurs by the posterior margin of the caudal vertebral body and the lamina or ligamentum flavum of the cranial level. This condition has been well explained as ‘the pincer effect’ of spinal cord compression (Fig. 50.5).16 As for the pathomechanism of cervical myelopathy in elderly patients, retrolisthesis of C4 occurs as a result of intervertebral disc degeneration and is one cause of spinal cord compression.17,18 In flexion of the cervical spine, the spinal cord must lengthen or move in an anterior direction in the spinal canal, resulting in axial tension. A bulging disc or anterior osteophytes can stretch the spinal cord in flexion. Anterolisthesis of the vertebral body can be a cause of spinal cord compression. These local conditions lead to the onset of myelopathy. The forward displacement of the spinal cord during flexion can bring about spinal cord dysfunction, even when cervical spondylosis is not present. Juvenile muscular atrophy of the distal upper extremity, which is called Hirayama disease,19 is considered to be a type of cervical myelopathy. In this disorder, findings of forward displacement of the dural sac and flattening of the lower cervical cord in a fully flexed neck have been shown on MRI.20
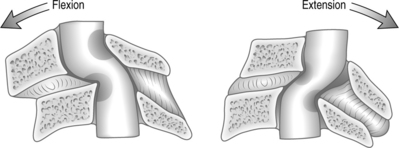
Fig. 50.5 Pincer effect of the spinal cord.
(Bernhardt M, Hynes RA, Blume HW, et al. Current concepts review. Cervical spondylotic myelopathy. J Bone Joint Surg 1993; 75A:119–128 with permission.)
It has been reported that some patients with athetoid cerebral palsy show cervical myelopathy at an early age (30–40 years of age).21 This is due to the excessive movement of the cervical spine. These exemplify the importance of dynamic factors in cervical cord dysfunction.
Ischemic factors
Spinal cord compression leads to ischemia in the spinal cord.22 Histopathological examination reveals the occurrence of ischemic injury in the gray matter and white matter in patients with myelopathy.9 In addition, several animal models have shown that disturbance in the vascular supply to the spinal cord plays an important role in the pathophysiology of spinal cord dysfunction.5
Ossification of the posterior longitudinal ligament
Ossification of the posterior longitudinal ligament (OPLL) (Fig. 50.6) often causes narrowing of the spinal canal due to the replacement of spinal ligamentous tissue by ectopic new bone formation.23 This disease is more common among Japanese and other Asians compared to Caucasians.24 The etiology of OPLL remains obscure; however, it has been reported that genetic background is a contributory factor. Recent studies using molecular biology have revealed that the collagen 11a2 gene (COL11A2),25,26 retinoic X receptor β gene (RXRβ)27 and nucleotide pyrophosphatase (NPPS) gene28 might be responsible for OPLL. It has been widely recognized that OPLL may cause severe myelopathy and radiculopathy. Ossification types of OPLL are classified into continuous type, segmental type, mixed type, and other types, according to the criteria proposed by the Investigation Committee on the Ossification of the Spinal Ligaments of the Japanese Ministry of Public Health and Welfare (Fig. 50.7)29 Among these types, myelopathy is frequently developed in the continuous or mixed types. OPLL progression is often observed in long-term follow-up after cervical laminoplasty and it can be a cause for the recurrence of myelopathy.30


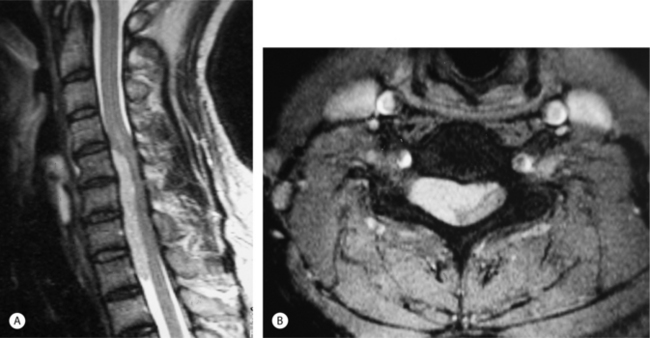
Cervical disc herniation
Cervical disc herniation (CDH) (Fig. 50.8) is one of the compressive lesions which might cause cervical myelopathy. It has been proposed that nuclear herniation or anulus protrusion compresses the spinal cord, but precise histopathological examinations have revealed that a disc herniation associated with the cartilaginous endplate is the predominant type of herniation in the cervical spine.31 The symptoms in patients with cervical disc herniation depend on the location of the herniated mass. A centrally located herniation mass, which is large enough to compress the spinal cord, produces cervical myelopathy, whereas laterally displaced herniation often leads to cervical radiculopathy. Patients with myelopathy due to disc herniation are relatively young, compared to those with cervical spondylotic myelopathy. The spinal canal is narrower in patients with myelopathy due to herniation than those with an asymptomatic central herniation. A history of cervical spinal trauma appears to be a predisposing factor for disc herniation.32 In some patients with the median and/or diffuse type of disc herniation, spontaneous regression of the herniated mass is observed on MRI.33 The symptoms often recover during such regression and therefore conservative treatment can be an option for mild myelopathy caused by cervical disc herniation.34
Adjacent disc disease after anterior cervical fusion
Although anterior cervical decompression and fusion is an established surgical procedure in the management of cervical lesions, numerous studies using long-term follow-up have revealed that adjacent disc disease could occur after fusion surgery (Fig. 50.9).35–38 In some cases, the adjacent disc disease leads to myelopathy in the long-term follow-up after anterior cervical fusion. Regarding the cause of the adjacent disc disease after anterior cervical fusion, it is believed that mechanical stress contributes to the disc degeneration at adjacent levels. A biomechanical study conducted by Matsunaga et al. demonstrated that shear strain of the adjacent segments had increased by on average 20% 1 year after surgery in the cases of double- or triple-level fusion.38

Calcification of the ligamentum flavum
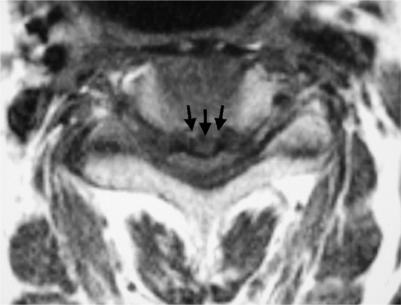
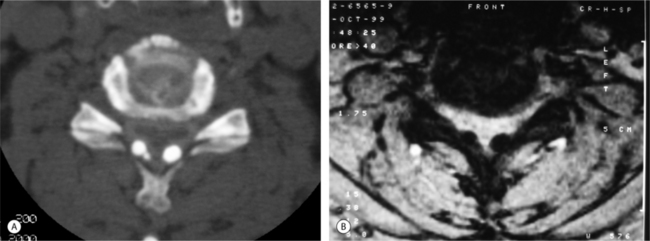
There have been a few cases reported in which calcification of the ligamentum flavum (CLF) (Fig. 50.10) narrows the spinal canal in the cervical spine, resulting in myelopathy. In the literature, most cases are Japanese,39 but one case was reported from the US.40 Kokubun et al. reported that 4% (11 patients) of 306 patients with cervical myelopathy in northern Japan had calcification of the ligamentum flavum.39 CT is the most useful diagnostic tool to detect this disease. Although the etiology is unknown, calcium phosphate deposition is observed in the pathology.
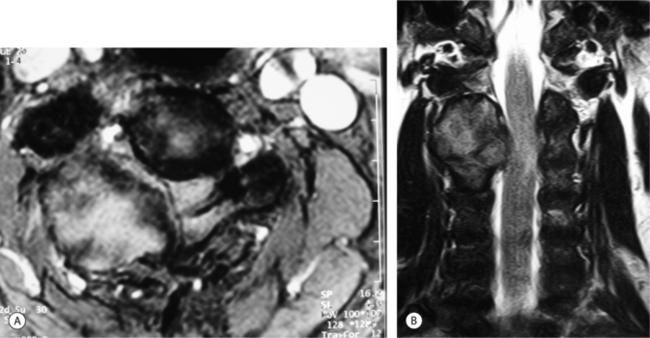
Rheumatoid arthritis
Involvement of the cervical spine in rheumatoid arthritis (RA) has been well studied.41–47 Compression of the spinal cord may result from direct compression by synovial pannnus or indirect compression due to cervical subluxation. Upper cervical lesions, identified as atlantoaxial subluxation (Fig. 50.11) and vertical subluxation (Fig. 50.12), can be causes of cervical myelopathy.47 The atlas dental interval (ADI) is a useful marker for the analysis of atlantoaxial subluxation. In patients with an ADI exceeding 5 mm, the space available for the spinal cord (SAC) is narrowed and they have an increased risk of cervical myelopathy if the space available for the cord is less than 14 mm (Fig. 50.13). As for the analysis of vertical subluxation (Fig. 50.14), several methods have been reported. McGregor’s line connects the posterior margin of the hard palate to the most caudal point of the occiput. The tip of the odontoid should not project more than 4.5 mm above this line. Ranawat baseline measurement is another method. Ranawat’s line is from the center of the sclerotic ring of C2 to the line between the center of the anterior and posterior arches of C1. A distance of less than 13 mm is abnormal. Lower cervical lesions, such as subaxial subluxation (Fig. 50.15) and swan neck or goose neck deformity, also are causes of myelopathy. Although the cervical spine is affected in 36–86% of patients with RA, the incidence of myelopathy is reported to be 4.9–32%.47 Regarding the neurological evaluation in patients with RA, Ranawat’s four-grade criteria are often used (Table. 50.2).48


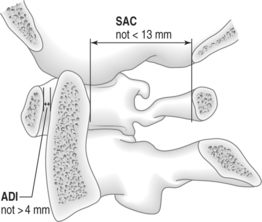
Fig. 50.13 Atlas dental interval (ADI) and space available for the spinal cord (SAC).
(Reprinted with permission from The Cervical Spine. 3rd edn. by the Cervical Spine Research Society Editorial Committee. Philadelphia: Lippincott-Raven; 1998.)
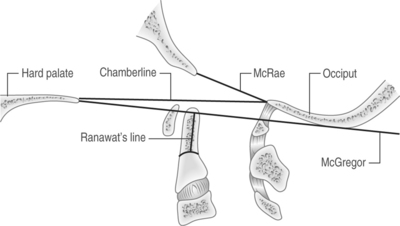
Fig. 50.14 Judgment of vertical subluxation.
(Reprinted with permission from The Cervical Spine. 3rd edn. by the Cervical Spine Research Society Editorial Committee. Philadelphia: Lippincott-Raven; 1998.)

Table 50.2 Ranawat’s Four-grade Criteria for the Neurological Evaluation in Patients with Rheumatoid Arthritis
| Class I | Pain, no neurological deficit |
| Class II | Subjective weakness, hyperreflexia, dysesthesias |
| Class III | Objective weakness, long-tract signs |
| Class IIIa | Ambulatory |
| Class IIIb | Nonambulatory |
Spinal tumors
Intradural extramedullary (IDEM) tumors might cause compressive myelopathy. Meningioma, neurofibroma, neurilemmoma, and schwannoma are common examples of IDEM tumors.49,50 Meningioma grows from the cells in the arachnoid (Fig. 50.16). Neurofibroma, neurilemmoma, and schwannoma usually arise from the dorsal sensory roots. Neurofibroma is accompanied by von Recklinghausen’s disease and sometimes follows the nerve root out of the spinal canal, resulting in a dumbbell-shaped tumor. IDEM tumors are typically eccentric and lead to Brown-Sequard type myelopathy. Gd-enhanced MRI is very useful to detect IDEM tumors. Metastasis to the cervical spine is another entity which might cause compression myelopathy, although such lesions are rare in the cervical spine (Fig. 50.17).51,52 The most likely primary tumors to metastasize to the cervical spine are from breast, prostate, and lung cancer. The primary site for metastasis is the vertebral body in the cervical spine. The symptoms of myelopathy are sometimes acute and gradually progressive. Kyphotic deformity due to vertebral collapse, direct tumor invasion in the epidural space, and insufficiency of the anterior spinal artery system might produce cervical myelopathy.
Epidural abscess
Spinal epidural abscess (Fig. 50.18) can cause a mass to develop in the spinal canal, leading to acute myelopathy.53,54 In patients with epidural abscess, fever and neck pain are usually observed. Staphylococcus aureus is the etiologic agent in over 50% of cases with acute epidural abscess. Spondylodiscitis may be accompanied as a local pathology, whereas epidural infection may occur hematogenously from a distant site.

Anomaly in the cervical spine
Anomalies in the cervical spine are frequently seen at the craniovertebral junction or at the upper cervical spine. In most patients, the anomalies are usually found in childhood as a congenital malformation; however, abnormal cervical structures in the cervical spine are sometimes found in adulthood. Among the anomalies in the cervical spine, myelopathy can be developed in the basilar impression, Arnold-Chiari malformation, and atlantoaxial instability associated with Down’s syndrome.55 Os odontoideum with instability also might cause myelopathy.56
Destructive spondyloarthropathy
Destructive change (Fig. 50.19) in the cervical spine is often seen in patients receiving long-term hemodialysis. The disease entity was first reported by Kunz et al. in 1984.57 Radiological features in this disease are disc space narrowing and irregularity of the cartilaginous endplate without osteophyte formation. The C5–6 level is involved in more than half of patients, but involvement of many levels is common. The prevalence of destructive spondyloarthropathy (DSA) is 4–20% in patients receiving hemodialysis and it increases in those who have long-term hemodialysis, longer than 10 years.58 The causes of myelopathy are cord compression due to spinal instability, intervertebral subluxation, intracanal amyloid deposition, and/or hypertrophy of the ligamentum flavum.59,60 Although the pathology of DSA has not been clearly elucidated, it has been reported that hyperparathyroidism and amyloidosis play an important role in the progression of DSA.59

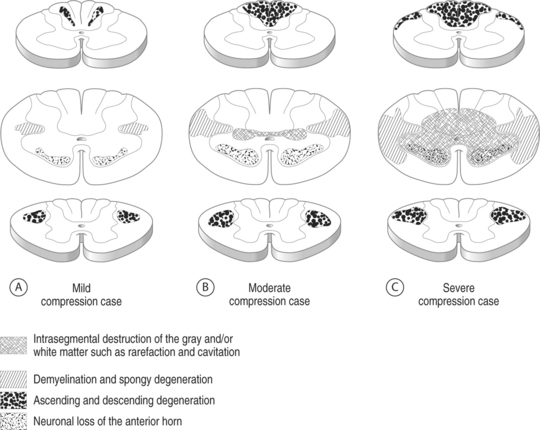
Pathological findings in the spinal cord under compressive conditions
In the macroscopic findings, the spinal cord with myelopathy shows anteroposterior flatness and it becomes atrophic due to compression. According to morphological studies using CT myelogram, the spinal cord sometimes reveals a boomerang shape or a triangular shape. Histopathological studies have shown that the damage of the neuronal components is mild in the spinal cord with a boomerang shape, while such damage is marked in cases with a triangular shape spinal cord.9 In addition, it has been reported that two parameters, anteroposterior compression ratio and the transverse area, are well correlated with spinal cord destruction and the recovery after decompressive surgery.61–63 The pathological change of the spinal cord is quite different depending on age, and extent and duration of compression. Ogino et al.64 reported the precise pathology of the spinal cord in patients with compressive myelopathy. Their study showed that in mild compression, limited demyelination and spongy degeneration are seen in the posterolateral white column, whereas in severe compression, extensive degeneration and infarction of the gray matter with diffuse degeneration of the lateral white columns are observed (Fig. 50.20). Further, severe cases always have accompanying developmental spinal stenosis. These pathological changes are not only localized at the most compressed site, but also at the craniocaudal regions in addition to the compression. Ascending degenerative demyelination is consistently seen in the cuneate and gracilis fasciculi of the posterior white columns in the spinal cord cranial to the compression site. Distinct descending demyelination of the lateral corticospinal tract is generally observed in the spinal cord caudal site.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


