Chapter 19 Bunion Deformity in Elite Athletes
Biomechanics of the First Metatarsophalangeal Joint
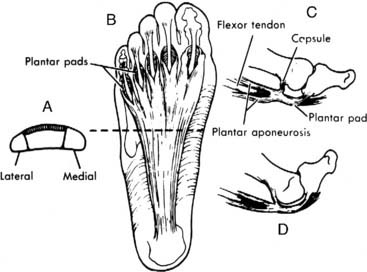
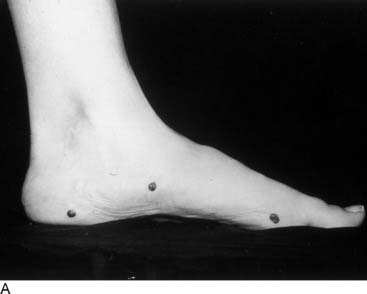
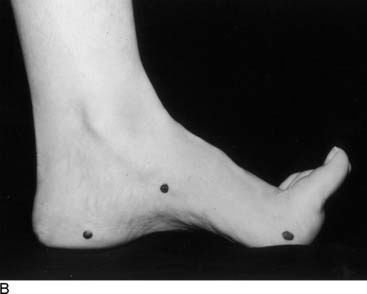
The main function of the first metatarsophalangeal joint is to stabilize the longitudinal arch through the windlass mechanism. Anatomically the windlass mechanism consists of the plantar fascia inserting into the base of the proximal phalanx via the plantar plate (Fig. 19-1). As the windlass mechanism becomes functional in the last half of stance by the dorsiflexion of the proximal phalanx on the metatarsal head, the metatarsals are depressed as weight is transferred to the toes. The effect of the windlass mechanism is greatest for the hallux and least for the small toe. Secondarily the windlass mechanism elevates the longitudinal arch and aids in inversion of the calcaneus (Fig. 19-2). When a hallux valgus deformity develops and lateral subluxation of the proximal phalanx on the metatarsal head occurs, the sesamoid sling is no longer beneath the first metatarsal head; therefore the windlass mechanism becomes less functional (Fig. 19-3). This is because when dorsiflexion of the phalanx occurs, plantarflexion of the metatarsal and weight transfer to the hallux are diminished resulting in progressive loss of the stability of the longitudinal arch. As it progresses, this loss of stability weakens the medial longitudinal arch, resulting in weight transfer from the first metatarsal to the second. This subsequently can result in excessive fatigue of the foot and possibly callus formation beneath the second metatarsal. This combination of effects results in diminished performance in the athlete, although it could be tolerated by the nonathlete.

Types of Hallux Valgus Deformity
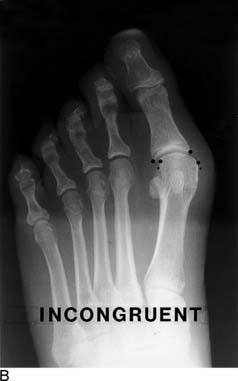
The hallux valgus deformity can be divided into two basic groups—persons with a congruent joint and those with a noncongruent or subluxed joint. In those with the congruent deformity, the windlass mechanism is not disrupted, and therefore the stability of the foot is not a problem (Fig. 19-4, A). In these individuals, the main disability is a large medial eminence, which results in chafing against their shoe. In the noncongruent deformity, there is progressive subluxation of the metatarsophalangeal joint that leads to instability and weight transfer (Fig. 19-4, B). In these individuals, the problem is more than an enlarged medial eminence because of the instability that occurs. If the enlarged medial eminence results in sufficient disability for the athlete and he or she can no longer function at the level needed to participate in his or her sport, a hallux valgus repair can be considered.

< div class='tao-gold-member'>
Related posts:
 Impingement Syndromes of the Foot and Ankle
Impingement Syndromes of the Foot and Ankle
 Ankle Sprains, Ankle Instability, and Syndesmosis Injuries
Ankle Sprains, Ankle Instability, and Syndesmosis Injuries
 Disorders of the Subtalar Joint, Including Subtalar Sprains and Tarsal Coalitions
Disorders of the Subtalar Joint, Including Subtalar Sprains and Tarsal Coalitions
 Assessment and Treatment of the Elite Athlete: Helpful Hints and Pertinent Pearls
Assessment and Treatment of the Elite Athlete: Helpful Hints and Pertinent Pearls
 Ankle and Midfoot Fractures and Dislocations
Ankle and Midfoot Fractures and Dislocations
 An International Perspective on the Foot and Ankle in Sports
An International Perspective on the Foot and Ankle in Sports



