How often does a child with BPBP have a permanent, incomplete recovery?
What are the limitations of the shoulder with an incomplete recovery?
What are the risks of glenohumeral deformity or dislocation?
What radiographic tests are used to assess the glenohumeral joint?
How is the deformity classified?
What surgical techniques are used to treat the adduction, internal rotation contracture, and ER weakness?
When is joint reduction indicated?
Which techniques are used for joint reduction and stabilization?
When are tendon transfers indicated?
What are the indications for a humeral osteotomy?
What are the long-term outcomes of these procedures? Expected complications?
are required. Through the radiographic advances of MRI scans, confirmed by ultrasound and arthrograms, it is clear that deformity starts very early in life and is progressive if untreated.
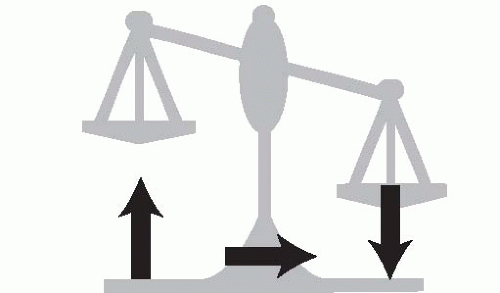 FIGURE 21-1 The return of internal rotator strength before ER muscle activity leads to an imbalance about the glenohumeral joint. This can progress to deformity and dislocation. |
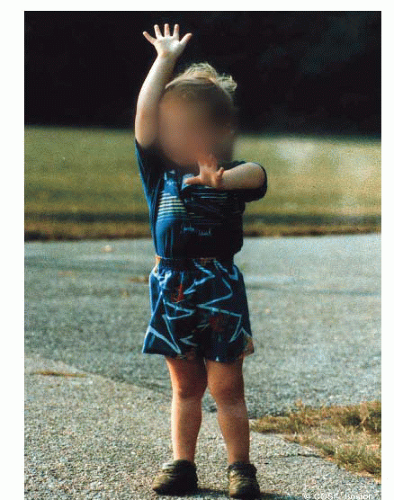 FIGURE 21-2 The affected left arm of this child with incomplete recovery reveals restrictions in ER and above horizontal shoulder function that is typical for these patients. He has to reach his mouth with his shoulder maximally abducted. He cannot reach the top of head and can only reach the left side by tilting his neck forward and to the side. His humeral head is dislocated. |
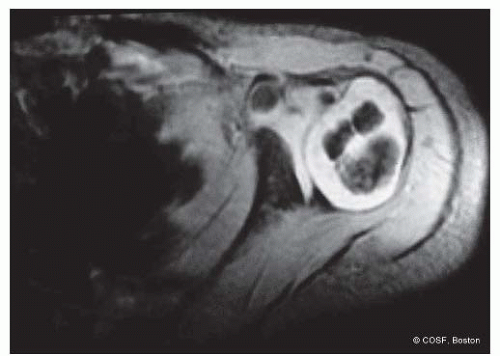 FIGURE 21-3 MRI of the affected glenohumeral joint reveals posterior subluxation of the humeral head and glenoid deformity with an early pseudoglenoid or biconcave joint. The humeral head is already beginning to change shape, and the position of the biceps insertion reveals the presence of an internal rotation contracture. |
Maintaining passive ER with scapular stabilization is integral to their therapy program. Conversely, those infants and children losing ER in adduction12 and/or abduction2 are most at risk for glenohumeral deformity (Figure 21-6). Before a fixed deformity develops, the shoulder instability can be palpated in the posterior soft spot with alternating internal (subluxation) and external (reduction) rotation. Later, the dislocated humeral head is palpable posteriorly with clear asymmetry to the opposite side anatomic situation (Figure 21-7). Scapular winging is present in all these children with muscle imbalance and contracture (Figure 21-8).
Table 21.1 Gilbert and Tassin’s modified MRC classification for motor strength | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
Table 21.2 Modified Mallet classification | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
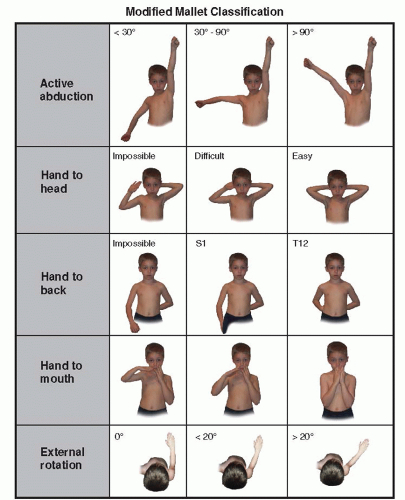 FIGURE 21-4 Modified Mallet classification for global abduction, ER, hand to neck, hand to spine, and hand to mouth. Each category is graded I to V with I, no function; V, normal function, and grades II, III, and IV depicted by illustration. Some children are not testable due to age and lack of cooperation at that particular visit. An aggregate Mallet score is a combination of the scores for all five categories, ranging 0 to 25. |
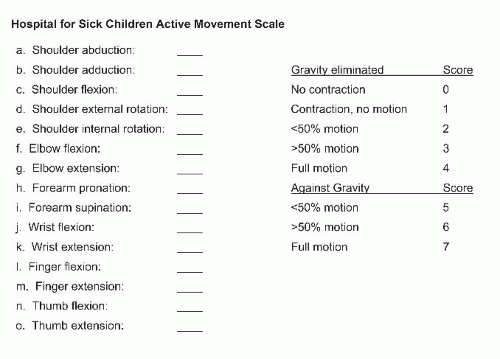 FIGURE 21-5 The Hospital For Sick Children Active Movement Scale grades each muscle movement from the shoulder to the hand by a score of 0 (no function) to 7 (normal function). A child must have full gravityassisted function (score of 4) before antigravity scoring can be obtained. |
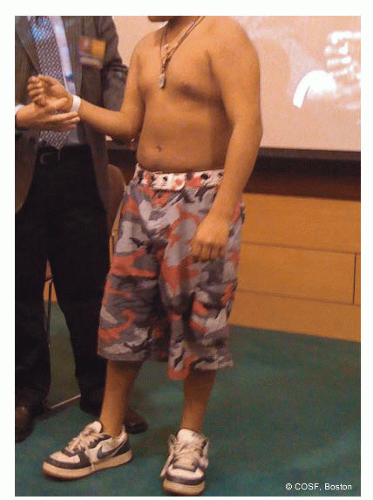 FIGURE 21-6 With the scapula stabilized, this patient has limited ER in adduction. The glenohumeral joint needs investigation for deformity. |
in developmental dysplasia. MRI scans are diagnostic (Figure 21-9).13 CT scans are faster, cheaper, and give comparable information as MRI scans but have high radiation dosing and do not show the unossified glenoid apophysis14,15 (Figures 21-10 and 21-11). Arthrograms also give comparable information16, 17, 18 and 19 (Figures 21-12 and 21-13). The clinical continuum of dysplasia at the glenohumeral joint progresses from anatomic alignment and symmetric development, increased glenoid retroversion, humeral head posterior subluxation, and biconcave or pseudoglenoid (Figure 21-14) to a frank dislocation with a flat humeral head and glenoid (Figures 21-15 and 21-16). The degree of deformity can guide the surgeon on timing and the type of operative intervention. MRI scans are more capable than physical examinations of revealing the presence and degree of glenohumeral dysplasia.
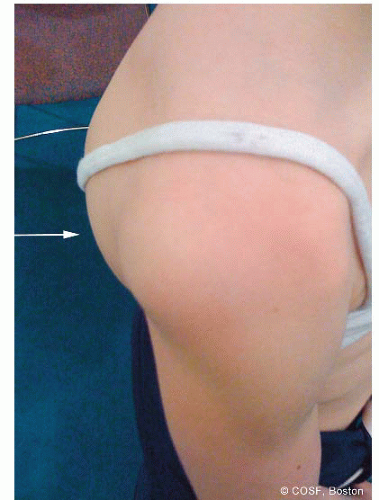 FIGURE 21-7 View of the affected right shoulder with obvious posterior dislocation of humeral head. |
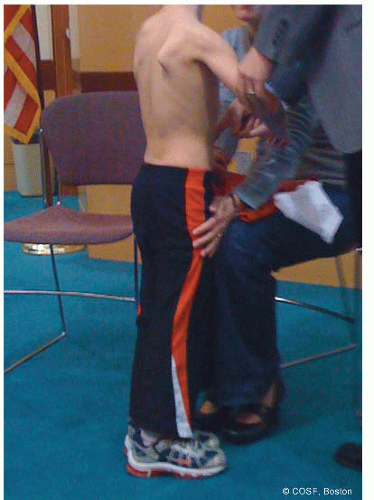 FIGURE 21-8 Marked scapular winging in this patient with dysplastic glenohumeral joint and shoulder contractures. |
 FIGURE 21-9 Obvious asymmetry between affected and unaffected glenohumeral joints by MRI scan. The affected side has marked glenoid deformity, posterior subluxation of the humeral head, and a pseudoglenoid. The unaffected side has anatomic alignment. |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


