How common is brachial plexus birth palsy (BPBP)?
Can we define the cause?
How do you distinguish an avulsion injury from an extraforaminal rupture?
What is the expected outcome by natural history?
What are the indications for nerve surgery?
What techniques are most commonly used for nerve reconstruction?
What are the expected outcomes and differences from both avulsion and extraforaminal reconstructions?
foramina will be empty. Distal to the neuroma, depending on the size of the neuroma and extent of injury, more normal individual divisions, cords, and/or nerves are isolated. Each situation is different and, accordingly, recognized, dissected, and recorded. The simple goal is to provide healthy neural input to affected muscles. The method by which this is achieved varies from case to case.
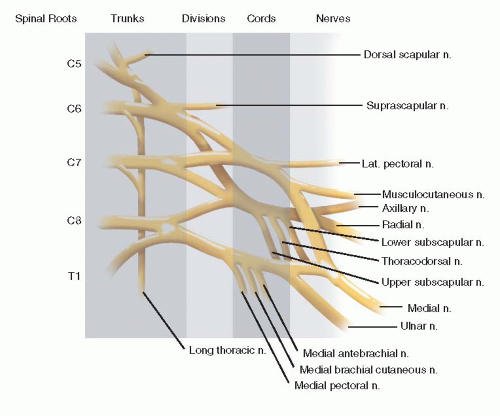 FIGURE 20-1 Normal anatomy of brachial plexus outlining nerve roots > trunks > cords > individual nerves. Obviously there are anatomic variations to this two-dimensional illustration, but this is the foundation of brachial plexus work. |
include congenital differences, central nervous system or spinal cord pathology, and infection.
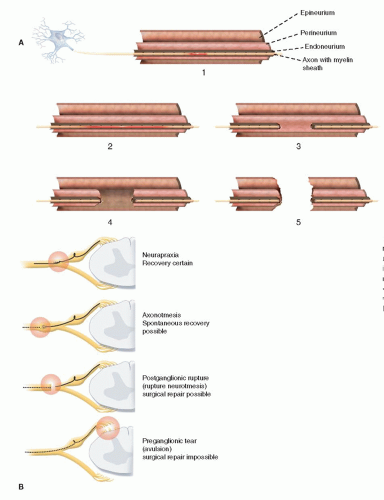 FIGURE 20-2 A: Sunderland classification of neural injury with neurapraxia (type 1 short segment and type 2 long segment neurapraxic injury), axonotmesis (type 3 disruption of nerve but perineurium and epineurium intact) while type 4 has disrupted perineurium and intact epineurium), and neurotmesis (type 5 with complete disruption of nerve). B: Sequence of nerve injuries from avulsion with no chance of recovery; to extraforaminal rupture with variable recovery (Sunderland type 3, and even 4); to nerve stretch (Sunderland types 1 and 2) with high likelihood of full recovery. |
the brain-spinal cord axis and the peripheral nerve muscle axis at each avulsion level.
 FIGURE 20-3 Horner syndrome with ptosis, miosis, enophthalmos, and anhidrosis. There is a high correlation between an avulsion injury and the presence of a Horner syndrome. |
 FIGURE 20-4 Typical posture of elbow extension (absent biceps), wrist flexion (absent wrist extensors), and digital flexion (absent finger extension). |
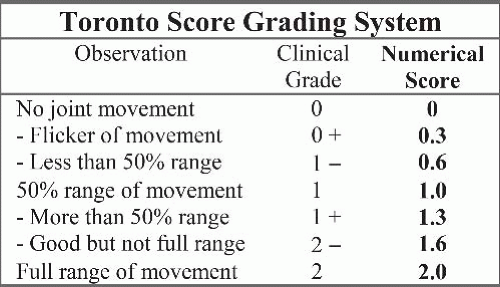 FIGURE 20-5 Toronto score for microsurgical indications. A score <3.5 is utilized in some centers as indicating nerve exploration and reconstruction. Others use the absence of biceps function as the indication for nerve surgery. Timing is debatable. |
long-term economic cost and outcome. We still do not have the definitive answers that can be applied to any given case. This ambiguity and lack of consensus complicates life for parents trying to decide what is best for their child’s future. The trends, however, are clear, and prospective study results are coming.
Table 20.1 Treatment recommendations in obstetric palsy | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||
Also, in infants there is a reasonable chance of some recovery of hand function. However, even the most experienced surgeons are challenged when there is a mismatch between what is needed and what is available for reconstruction.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


