This chapter will review what is currently known about bone health in the female athlete, including assessment techniques and various factors that impact bone health—both positively (such as exercise) and negatively (including the Female Athlete Triad) (Figure 6.1). Strategies for optimizing bone mineral density at all ages will be discussed.
Figure 6.1 Normally, regular weight-bearing activity such as running is osteogenic. However, menstrual dysfunction associated with low energy availability may compromise optimal bone mineral density. Courtesy of the International Olympic Committee.
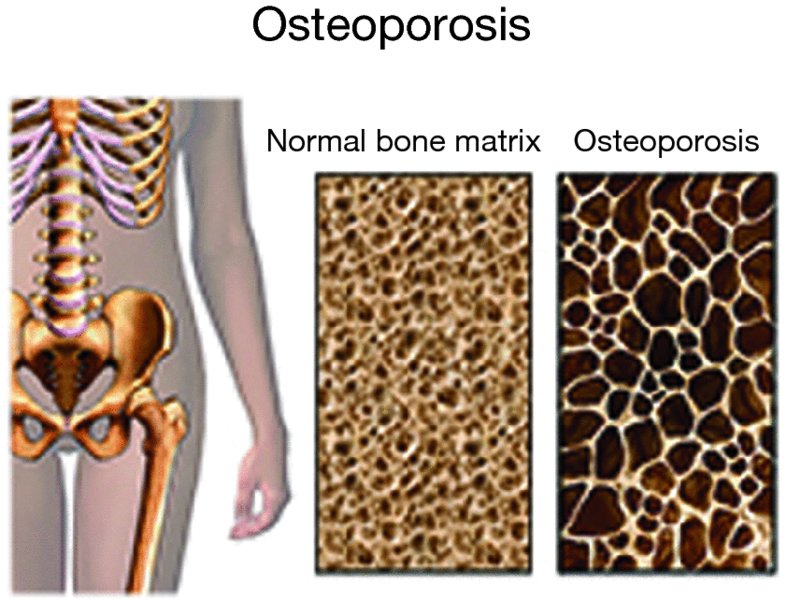
Bone is an active tissue composed of connective tissue fibers, as well as various proteins and calcium–phosphorus deposits, all of which give it strength and resistance to varying degrees of loads. The skeleton is comprised mainly of two types of bone tissues—dense bone tissue (compact bone), found primarily in the outer part of cylindrical long bones, and spongy bone tissue (trabecular bone) that includes many spaces that give it the appearance of a sponge. As bone ages, the amount of bone is decreased and the structural integrity of trabecular bone is impaired. In addition, cortical bone becomes more porous and thinner. These changes make the bone weaker and more likely to fracture (Figure 6.2).
The strength of the bone is the most important measure to its quality and is affected by a number of components:
Bone mineral density (BMD)
Bone size (geometry)
Micro-architectural structure of the bone
Collagen and other proteins (provide hardness and flexibility to the skeleton)
Bone metabolism—the turnover rate of bone tissue
Bone density itself accounts for about 70% of bone strength, and below a certain threshold, it may lead to osteopenia or osteoporosis.
The World Health Organization (WHO) has defined osteopenia as BMD between 1.0 and 2.5 standard deviations (SD) below normal, and osteoporosis as below 2.5 SD. The T-score relates to the score as compared with a 30-year-old woman, while the Z-score compares a woman’s results to those women of her own age. These definitions were developed for the evaluation and management of postmenopausal women with low bone density and are frequently used as decision points for initiation of treatment.
There are several methods for assessing bone density status. The most common methods in clinical practice and research today are as follows:
Dual X-ray absorptiometry (DXA)—This is a simple, reliable test, with high repeatability that is suitable for predicting osteoporotic fractures. It is the only test that has been validated for osteoporosis diagnosis. The main disadvantage of this method is that it does not reflect other important factors affecting bone strength, such as size, architecture, geometry, and elastic properties. Another drawback is it is actually a 2-dimensional measurement and therefore can be confounded by vertebral body size, and surrounding soft tissues leading to measurement errors.
Quantitative computed tomography (QCT)—This method allows 3-dimensional measurements of both trabecular bone and cortical bone, which assesses bone density with a greater accuracy than the DXA. The main disadvantages to this method are its low availability, high price, and the high radiation doses involved. Axial QCT is used for the spine and hip, while peripheral QCT (pQCT) can be used in the peripheral skeleton, such as the distal radius and tibia. The latter (pQCT) has a lower dose of radiation.
Quantitative ultra sound (QUS)—This technology is free of ionizing radiation, and is able to characterize important mechanical indices of bone (such as elasticity) that contribute to strength and resistance to fractures. Measurements are generally done at the calcaneus, generating two different parameters: the speed of sound (SOS) and broadband ultrasound attentuation (BUA). More sophisticated QUS indices can be derived from these two basic measures. The machines are compact and also relatively inexpensive. For these reasons, this assessment technique is sometimes used in initial screening for osteoporosis. There is a reasonable correlation with DXA, especially in postmenopausal women, but the correlation is not as good for predicting fractures. Another disadvantage is that QUS technology cannot measure the spine or hip, and it has lower repeatability; thus, it is not suitable for tracking changes over time.
Bone is a dynamic tissue. The acquisition of bone that occurs during childhood and adolescence accounts for 90% of adult bone mass. Bone mineral density is influenced by a number of intrinsic and extrinsic factors:
Intrinsic factors:
Genetics—Between 60–90% of the variability in ultimate peak BMC is attributable to genetic factors. This also accounts for other bone health parameters such as bone geometry, bone turn-over markers, and risk for osteoporotic fractures.
Sex—Women have lower BMD than men. Men however can also suffer from osteoporosis, under certain circumstances.
Age—BMD increases until the third decade and decreases gradually from the 5th decade of life onward in both sexes. There is an additional rapid decrease in the few years immediately during and after menopause, especially in trabecular bone (Figure 6.3).
Body size—People with low body weight and tiny bones have lower stimuli for bone mechanical loading and therefore lower BMD.
Race and ethnicity—White and Asian women have lower BMD as compared with Hispanic and African-American women.
Family history of osteoporosis and osteoporotic fractures is a strong predictor of low BMD and eventual fractures.
Extrinsic (environmental) factors:
Body weight—Body mass index is correlated with BMD. Both lean body mass as well as fat mass (which affects hormonal status, i.e., increases calcium absorption, reduces sensitivity to parathyroid hormone, etc.) have positive effects on bone density.
Diet—Calcium and vitamin D are the most significant components in the diet that may affect bone mass. Other nutrients have been studied as having an effect of the bone status. These include dietary fibers, caffeine, alcohol, phosphorus, vitamin K, protein, sodium, and more.
Increased consumption of dietary fibers (over 30 grams per day) may interfere with the absorption of calcium, but this issue is considered negligible due to the relatively low fiber intake in the general population.
Daily consumption of beverages containing caffeine (several cups/day) may cause an increased loss of calcium in urine. Researchers do not agree about the effect of increased consumption of caffeine on bone density. Caffeine seems to have little impact, if any, on calcium and bone density in people who meet the daily calcium intake recommendations.
Alcohol—Increased consumption is a common cause of secondary osteoporosis through an increase in the incidence of fractures and complications in their recovery.
Exercise— The specific effects of physical activity on bone health have been investigated in randomized clinical trials and observational studies. According to Wolff’s law, bone reacts proportionally to the forces implied to it. The forces include compression forces from gravity, loads placed upon the bone with activity, and pulling forces at the tendon interface. Mechanical loading in childhood and during adolescence positively affects bone health in adulthood and decreases osteoporotic fractures, probably by increasing peak bone mass, whereas inactivity is associated with lower bone mass. Physical activity needs to be continuous throughout life in order to maintain the peak bone mass achieved and to prevent bone loss at any age. The osteogenic effect of physical activity on bone is especially prominent in high-impact sports such as running, jumping, and ball games. On the other hand, swimming and cycling, which are nonimpact sports (non-weight bearing) do not affect bone density much. The effect of physical activity on bone mass depends also on the specific sites of impact of the various sport activities and therefore varies between bones. In tennis or squash players, for instance, upper extremity BMD is significantly higher on the dominant side compared with the nondominant side, especially if the athlete started playing at a younger age—premenarchal. It appears that calcium intake especially during childhood, acts synergistically with physical activity to promote bone health, but physical activity has a larger osteogenic effect compared with calcium intake.
Sex hormones—Sex steroids secreted during puberty substantially increase BMD and peak bone mass. Estrogen is osteoprotective, primarily through its action to inhibit bone resorption. It also facilitates Vitamin-D-related intestinal calcium absorption. Progesterone is thought by some researchers to have a role in stimulating bone formation. In adolescents and young women, the sustained production of estrogen is essential for the maintenance of bone mass. Reduction in estrogen production with menopause is the major cause of loss of BMD during later life. Timing of menarche (late menarche), absent or infrequent menstrual cycles, and the timing of menopause (early menopause) influence both the attainment of peak bone mass and the preservation of BMD. Testosterone has an anabolic effect on bone. Testosterone stimulates osteoblasts, and through its aromatization to estrogen, may also inhibit osteoclastic activity.
Other hormones
Only gold members can continue reading. Log In or Register to continue