9
Bone Healing
Robert C. Manske and Gary A. Shankman
1. Identify and describe the phases of bone healing.
2. Discuss the objectives that serve as the foundation of fracture management and bone healing.
3. Define osteoblasts, osteoclasts, and osteocytes.
4. Define and discuss Wolff’s law.
5. Discuss stress deprivation, immobilization, and normal physiologic stress as they apply to fracture healing.
6. Define three complications of bone healing.
7. Outline and describe six areas of descriptive organization of classifying fractures.
8. Describe the five types of pediatric fractures defined by Salter-Harris.
9. Define pathologic fractures and list four types.
10. Discuss how osteoporosis affects fractures.
12. List common methods of fracture fixation, fixation devices, and fracture classifications.
13. Discuss clinical applications of rehabilitation techniques used during bone healing.
STRUCTURE AND FUNCTION
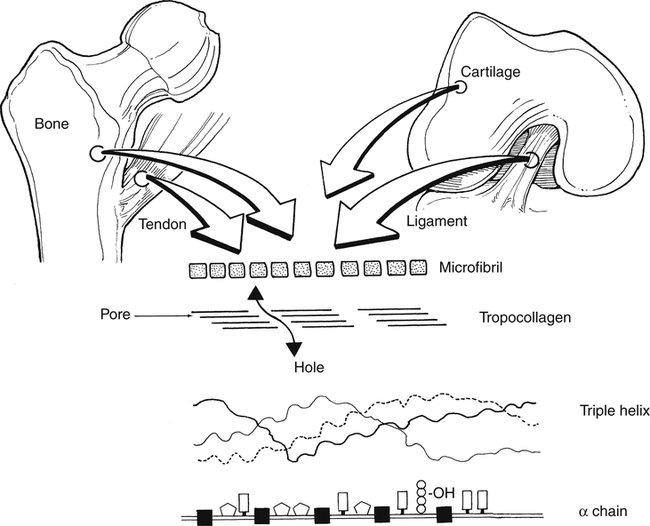
Bone is an intense metabolically active tissue. Bone has unique mechanical characteristics that are determined primarily by the structural components of bone tissue. Chemically complex, bone tissue is approximately 65% mineral and 35% organic matrix. The major organic constituent of bone is type I collagen, representing about 90% of the dry weight of bone.35 The remaining 10% is composed of noncollagenous matrix proteins, lipids, phospholipids, proteoglycans, and phosphoproteins. The principal inorganic component of bone is a crystalline calcium phosphate hydroxyapatite.35 This compound is generally brittle, tolerating only small amounts of deformation before fracture. The remaining tissue volume includes fluid-filled vascular channels and cellular spaces.12
Bone Cells
There are three types of bone cells. Osteoblasts are functionally distinct cells that form bone matrix (osteoid) and synthesize type I collagen,35 and are commonly found on a bony surface. These cells are unique in that they have a large volume of endoplasmic reticulum, Golgi apparatus, and mitochondria to synthesize collagen and secrete matrix proteins.35
Osteoblasts and osteocytes are distinguished more by their location than by their structure and function.15 Osteoblasts are responsible for synthesis, deposition, and mineralization of bone. They are derived from bone marrow and secrete procollagen on all active bone surfaces. Once the osteoblast is done forming bone, it can become an osteocyte.
Osteocytes actually are osteoblasts that are embedded within newly formed mineralized bone matrix.35 Chemically, osteocytes differ from osteoblasts in that they demonstrate fewer organelles and a greater nucleus to cytoplasmic ratio.35 These cells represent approximately 90% of mature skeletal tissue and metabolically function to control extracellular concentrations of calcium and phosphorus.35 Osteoid osteocyte, and osteocytic osteoblasts are cells that are in an intermediate changeover from osteoblast to osteocyte, thus the pure distinction between cells may be more related to developmental stage than differing cell types.37
Osteoclasts are giant cell multinucleated bone resorption cells. Osteoclasts synthesize a specific acid phosphatase enzyme and also produce hydrogen ions, which in turn lower the pH environment.35 The reduced pH increases the solubility of the crystalline phosphate-hydroxyapatite that functions to remove the organic matrix crystals via acid proteolytic degradation.35 These enzymes remove a thick layer of osteoid covering, allowing osteoclasts to bind to bone and begin resorption if needed.5
Types of Bone
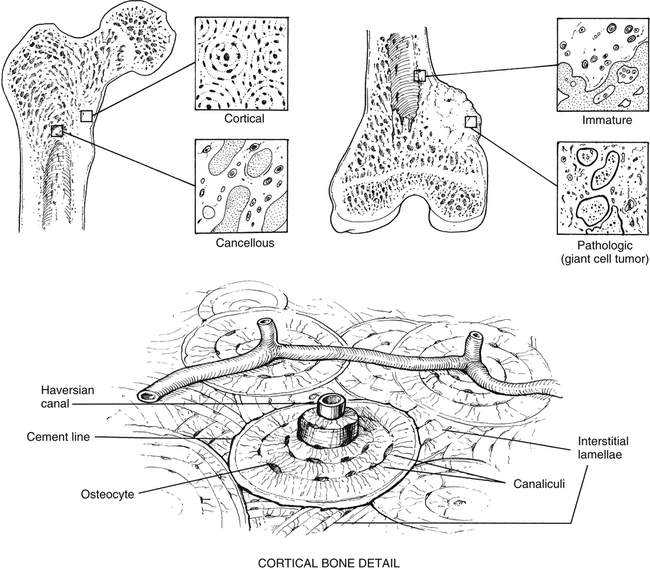
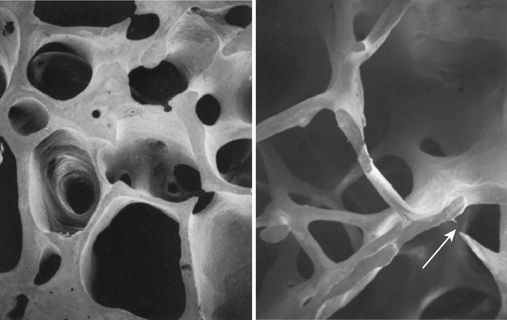
The microscopic organization and classification of bone tissue involves two distinct forms that change or adapt as we age: (1) normal, mature lamellar bone; and (2) weak, fragile, immature woven bone (Fig. 9-1).
Woven bone is structurally immature, embryologically (primary) fragile, and weak with a random disorganized collagen arrangement.3 This random arrangement of collagen fibers allows strength in all directions, while preferring strength in none specifically. Therefore this form of bone is not nearly as strong as mature bone. This specific type of bone is more commonly seen in embryos and newborns, but can also be seen in the adult during fracture repair callus, bone tumors, and various bone pathologies.35
One of the unique features of woven bone is that it can be deposited without any previous part of a cartilaginous model existing.23 Woven bone’s primary function is to provide temporary, quick acting mechanical support for injured skeletal tissue.
Very early after birth (approximately 2 months to 4 years), woven bone slowly remodels into organized, structurally mature lamellar bone. A clinically relevant feature of woven bone is that its specific mechanical behavior is termed isotropic; that is, woven bone does not conform to Wolff’s law, so its biomechanical reactions to applied forces and stress is similar in all planes.3 The disorganized arrangement of collagen fibers in woven bone strongly contributes to this unique characteristic (Fig. 9-2).3
Lamellar bone refers to mature remodeled woven bone. Mature bone begins formation at about 1 month after birth11 and comprises most of the skeleton by age 4 years.2 The collagen arrangement in lamellar bone is highly structured and organized. This gives normal mature lamellar bone anisotropic mechanical properties that are stress oriented, which characteristically respond to Wolff’s law.3
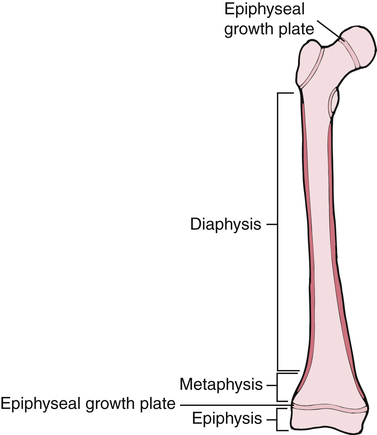
Bones are not only classified into various types, but also by their shape. Long bones are considered to have greater length than width. Examples of long bones are the femur and the humerus. These bones are tube shaped with widening at each end. Long bones have a diaphysis, which is the tubular shaped midportion that houses cancellous bone and the intermedullary canal where blood cells are formed (Fig. 9-3). The proximal and distal ends of the long bone widen to form a metaphysis, which continues to widen even more into the epiphysis or the end of the bone. In growing children, before skeletal maturity, the metaphysis and the epiphysis are separated by an epiphyseal growth plate. This can be a common area of fracture before skeletal maturity, at which time the two ends fuse and demarcation is not detectable.
Macroscopic Structure of Bone
Osseous tissue is structurally organized as either cancellous (trabecular bone) or cortical bone (compact bone). Cancellous bone is located at the metaphysis of long bones, as well as the vertebrae and other cuboid bones.3
Cortical bone, also known as compact bone, is located in the diaphyseal portion of long bones. Compact bone is very dense and hard on all surfaces, allowing it to function both structurally and for protection. Approximately 80% to 90% of the volume of cortical bone is calcium.17 The major structural subunit of cortical-compact bone is the osteon. As described by Bostrom and colleagues,3 the osteon is a central component of the haversian system.
Haversian bone is the most complex type of cortical bone. It is composed of vascular channels circumferentially surrounded by lamellar bone. This complex arrangement of bone around the vascular channel is called the osteon. The osteon is an irregular, branching, and anastomosing cylinder composed of a more or less centrally placed neurovascular canal surrounded by cell permeated layers of bone matrix.3 Primary osteons are those that develop into mature bone, while as new haversian canals are constantly formed, secondary osteons form on top of the old. Conversely, trabecular or cancellous bone is uniformly less dense with a large surface area and is significantly metabolically more “active” than cortical bone.3 In fact, even though cortical bone (compact bone) has four times the mass of trabecular bone, the metabolic activity of trabecular bone is eight times greater than that of cortical bone.3 Because bone turnover is a surface-oriented event, the profound surface area of trabecular bone explains the greater cellular exchange of cancellous bone.3
Bone Remodeling
The phenomenon of cellular turnover or remodeling of bone is a process that occurs on the surface of various portions of bone (periosteal, endosteal, trabecular, and haversian canal).35 Generally, bone remodeling is a lifelong activity that responds to mechanical stress (torsion bending, compression, tension) according to Wolff’s law.3 In simplified terms, Wolff’s law states that intermittent physiologic loads applied to bone stimulate adaptive responses. Removal of mechanical forces on the bone has the opposite effect. That is, when bone does not receive appropriate physiologic stress, osteoclastic activity overwhelms osteoblast production, which in turn reduces bone mass. The Hueter-Volkmann law is the reverse of Wolff’s law and is more specifically applied to compression and tensile forces acting on physeal growth plates. Simply stated, this law suggests that compression forces limit bone growth, whereas tensile stress stimulates growth.3
Vascular Supply to Bone
The adult skeletal system receives between 5% and 10% of the body’s total cardiac output.35 Bone receives blood supply from three distinct but interconnected systems: (1) the nutrient artery, (2) metaphyseal–epiphyseal system, and (3) periosteal systems (Fig. 9-4).
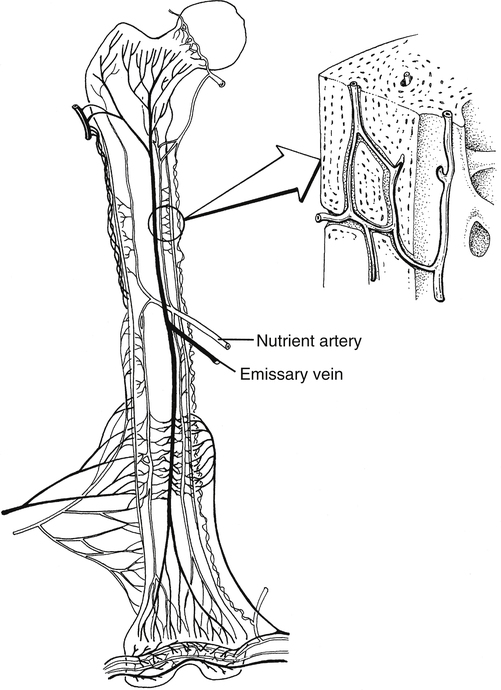
The arterial vascular system provides the origin of the nutrient system via a nutrient foramen in the diaphysis of long bones. The total number of nutrient vessels and foramen varies with each bone.3 The nutrient arteries enter the medullary space, then ascend and descend into the arterioles within the endosteal surface supplying the diaphyseal area of long bones.3 The metaphyseal–epiphyseal system is supplied by a periarticular complex system of the genicular arteries that penetrates the thin cortices of the metaphysis of long bones.3 Muscular attachment to the periosteal cortical sites of bone provides nutrition through the periosteal capillary system.3
Fractures, internal fixation devices, external fixation, and prosthetic joint implants devitalize the microcirculation of the cortical–periosteal and endosteal portion of the bone. The resultant ischemia of bone can lead to nonunion and bone infections.3 These important clinical ramifications of bone circulation disruption are evident when initiating therapeutic interventions of early weight bearing and closed kinetic chain (CKC) resistance exercise after fractures or joint replacement.
OSTEOPOROSIS
Osteoporosis is an age-related heterogeneous bone disease characterized by decreased bone tissue. Osteoporosis occurs when osteoblast (bone formation) activity is surpassed by osteoclast (bone resorption) activity (Fig. 9-5).21 This creates weaker bones that are subjected to greater rates of fracture. More than 1 million fractures a year can be attributed to osteoporosis27; vertebral body compression fractures are the most common.
Causes of osteoporosis may be multifactorial, including hormonal alterations following menopause, prolonged immobilization, diseases, and prolonged steroid administration. Women are at greater risk for developing osteoporosis for several reasons. Age-related cortical bone loss generally begins at about age 40 years,21 with the rate thereafter being approximately 0.5% annually for both men and women. However, because of lowered estrogen during menopause,21 women lose bone at a rate of 2% to 8% annually, resulting in a much greater total loss.
Poor absorption of calcium that leads to decreased bone mineralization is called osteomalacia.27 Causes include calcium-deficient diet, accelerated calcium loss, and malabsorption of calcium.21 Femoral neck fractures are common in patients with osteomalacia.27
A frail, elderly woman with osteoporosis suffers resultant multilevel thoracic vertebral body compression fractures. Bed rest with relative immobilization is ordered. She suffers further decrease in bone strength caused by immobilization. Rehabilitation is complicated by osteoporosis and fractures. Combined with the general overall negative effects of immobilization on the body’s systems, the effects of immobilization on the remaining skeletal tissue interfere with exercise, sitting, progressive ambulation, and functional activities, forming a vicious cycle that will need to be broken in order for a functional recovery.
CLASSIFICATIONS OF FRACTURES
By definition a fracture is any abnormal disruption in the normal anatomic continuity of bone. Therefore the classification of fractures takes into account the following criteria32,33:
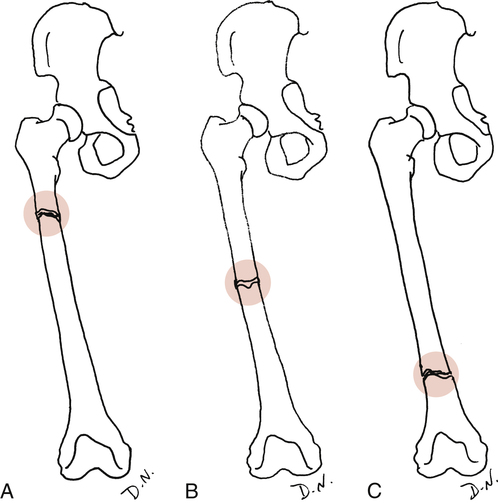
 Site of injury: The area of insult on the bone itself. An epiphyseal fracture describes the site, as does an intraarticular fracture or diaphyseal (shaft) fracture. Generally the site is described as the proximal, middle, or distal portion of a bone (Fig. 9-6).
Site of injury: The area of insult on the bone itself. An epiphyseal fracture describes the site, as does an intraarticular fracture or diaphyseal (shaft) fracture. Generally the site is described as the proximal, middle, or distal portion of a bone (Fig. 9-6).
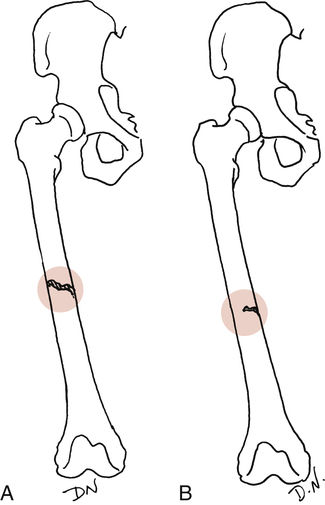
 Extent of injury: Complete or incomplete (Fig. 9-7). As the name implies, a complete fracture traverses the bone entirely. Incomplete fractures are commonly described as hairline cracks or greenstick fractures.
Extent of injury: Complete or incomplete (Fig. 9-7). As the name implies, a complete fracture traverses the bone entirely. Incomplete fractures are commonly described as hairline cracks or greenstick fractures.



Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


