Bone and Soft Tissue Tumors 
The musculoskeletal system is affected by a variety of (benign and malignant) tumors and tumor-like conditions that involve bones, joints, muscles, soft tissues, and peripheral nerves. Tumor-like conditions may be related to traumatic, infectious, arthritic, or developmental etiologies that lead to the development of soft tissue or bony mass-like lesions, which mimic neoplasia. Systematic assessment of the above lesions, correlation with plain films, and description in a structured reporting format are very useful to arrive at a definitive diagnosis (or the most relevant differential diagnosis), and to decide upon further management, including biopsy, surgery, and follow-up strategies. For appropriate imaging analysis and structured reporting, the lesions can be separately described using different templates for bone tumors and soft tissue tumors, depending upon the predominant respective tissue involvement and epicenter of the lesions. The checklist for structured reporting is outlined in Appendices 1–4 with samples of normal templates and abnormal (positive) reports. Conceptual details of related MR physics and imaging protocol are discussed in the chapter on MR protocol optimization.
 IMAGE EVALUATION
IMAGE EVALUATION
The below-outlined stepwise interpretation approach is only a practical guide, and all bone and soft tissue structures should be evaluated in multiple planes for their optimal assessment. The following discussion will help reader perceive which lesion characteristics are best depicted/evaluated in which particular plane.
1. The traditional tumor MR imaging protocols include one or two long-axis T1-weighted (T1W) images and three plane fluid-sensitive fat-suppressed T2-weighted (fsT2W) or short-tau inversion recovery (STIR) images. Most examinations include pre- and post-contrast evaluation in multiple planes or isotropic three-dimensional (3D) T1-weighted (T1W) gradient-echo images, which can be reconstructed in multiple planes. Recently, many tertiary care centers have incorporated diffusion-weighted (DW) and chemical shift (CS) imaging to evaluate the amount of diffusion restriction (e.g., cellularity by measuring apparent diffusion coefficient [ADC] value) and the presence of microscopic intralesional fat (benignity suggested by >20% relative loss of signal in bony lesions on out-of-phase imaging), respectively. MR angiography can be added in the protocol to assess the vascularity (vascular involvement, enhancement pattern) of neoplasms. The modality is particularly used in the preoperative imaging of sarcomas.
2. If available, plain film, US and/or CT findings should be correlated with MR features (Fig.1). The former modalities can be used for detecting presence of fat, calcification, bony cortex integrity, and periosteal reaction. MR imaging is beneficial for characterization of the bone marrow; however, the MR features of osseous lesions may sometimes confuse the reader, and clearly benign or indolent lesions on radiographs may occasionally appear aggressive on MR images. The diagnosis of bone lesions should be preferably based on radiographs and/or CT whereas MR imaging can be employed for further characterization, and definition of their extent.
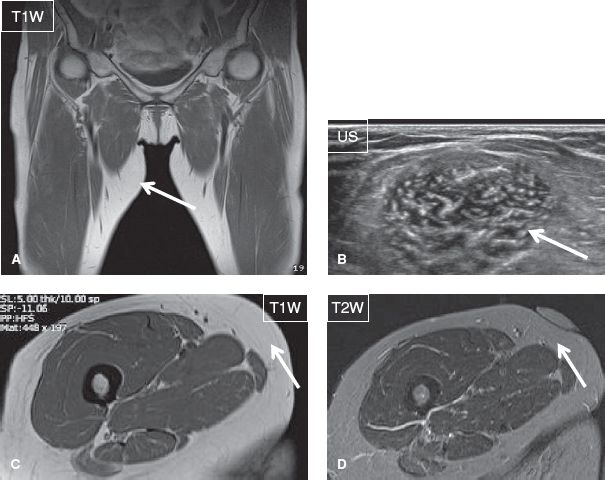
Fig. 1: Simple lipoma. Medial thigh palpable mass. Coronal (A) and axial (C, D) MR images and corresponding focused ultrasound image (B) show a purely fat-containing lesion (arrows) with a thin capsule in the medial proximal thigh at the site of the marker, consistent with a lipoma.
3. On MR imaging, the initial evaluation is performed on long-axis images to grossly assess the presence/absence of the lesion, its size, regional major soft tissue involvement, joint involvement, and presence or absence of skip lesions. Typically, lesions with elongated shape, and associated marked fascial and soft tissue edema, fascial or subperiosteal fluid, and/or sinus tract are infectious in etiology. The neoplasms do not produce much fascial edematous or fluid-like changes unless they are markedly aggressive with extra-compartmental extension. The appearance of the lesion is further characterized on T1W and T2W images to identify the predominant tissue composition, such as fat (T1 and T2 bright), fibrous (T1 and T2 dark), fluid or myxoid (T1 dark and T2 bright), cartilage (T1 intermediate and T2 bright), hemorrhage (T1 bright and T2 mixed), or calcification/osseous component (predominantly T1 and T2 dark ± internal fatty marrow elements).
4. Line up the axial T1W, T2W, pre- and post-contrast T1W (and subtraction, if available) images and synchronize them for tandem evaluation. If 3D (isotropic) T1W or T2W sequences have been obtained, the technologists should create reconstructions in prespecified axial, coronal, and sagittal planes to save reading time. Axial planes are ideal for the following purposes:
 Evaluating the internal characteristics of lesions, such as the predominant type of tissue, internal hemorrhage, calcification, fibrosis, necrosis, fluid–fluid levels, myxoid or cystic changes, etc.
Evaluating the internal characteristics of lesions, such as the predominant type of tissue, internal hemorrhage, calcification, fibrosis, necrosis, fluid–fluid levels, myxoid or cystic changes, etc.
 Determining the amount of cortical erosion or endosteal scalloping.
Determining the amount of cortical erosion or endosteal scalloping.
 Defining the intra- or extracompartmental location and potential intra-articular extension of the lesions.
Defining the intra- or extracompartmental location and potential intra-articular extension of the lesions.
 Assessing the involvement of neurovascular bundles.
Assessing the involvement of neurovascular bundles.
5. If CS imaging is available, check for either relative (>20%) signal loss in the bone lesion on out-of-phase images, which would indicate presence of microscopic fat and likely benignity of a marrow lesion; or for relative signal loss on in-phase images in the soft tissue lesions, which signifies presence of hemorrhage, such as in pigmented villonodular synovitis (PVNS). If DW imaging is available, check the ADC values as well as the presence and amount of diffusion restriction. Low ADC values (<1.1× 10−3 mm2/s) are seen with highly cellular, potentially malignant lesions, whereas high ADC values are seen with lower cellularity, probable benign or low-grade lesions. Evaluate CS and DW images in conjunction with the conventional images, e.g., fatty metamorphosis or fibrosis of lesion following successful treatment will also restrict diffusion. Finally, if time-resolved MR angiography has been performed, evaluate the degree increased or decreased regional vascularity, and perfusion of the lesion apart from patency of regional vessels for preoperative mapping. Fast and early uptake and/or wash out of contrast from the lesion indicate an aggressive vascularized lesion, and the potential responsiveness of the latter to radiation treatment. Post-treatment evaluation for residual or recurrent lesion is also better performed using time-resolved MR angiography and pre- as well as post-contrast delayed imaging, as part of the tumor imaging protocol. One would see early blush of nodular contrast enhancement with residual/recurrent disease, while gradual mild diffuse fill-in of contrast would be observed in post-radiation granulation tissue and scar tissue.
6. After filling the structured report, compile the imaging (MR, CT, plain film) findings together to indicate whether the lesion is benign (e.g., ganglion, lipoma, vascular malformation, nonossifying fibroma (NOF), cortical avulsive deformity, and unicameral bone cyst; Figs. 1–6); indeterminate (e.g., solid or centrally enhancing soft tissue lesion, bony lesion with ill-defined margins and/or periostitis; Fig. 7); or clearly malignant, unless proven otherwise (e.g., infiltrative soft tissue mass extending into different compartments, large heterogeneous necrotic mass, and bony lesion with cortical erosion and soft tissue mass; Fig. 8). Table 1 provides useful guides for differentiating between malignant and benign musculoskeletal lesions whereas Table 2 illustrates the differential diagnosis of various benign entities based on their specific tissue characteristics and locations in soft tissues.
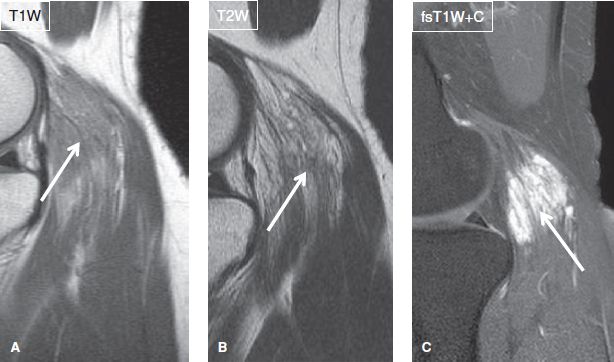
Fig. 2: Intramuscular hemangioma in a 27-year-old woman, who presented with a tender mass in the popliteal region. Sagittal images. A, B: The noncontrast images demonstrate multiple linear strandy areas of fat signal (arrows) within the gastrocnemius muscle with bubbly hyperintensities, without associated architectural distortion or other aggressive features. C: The postcontrast image reveals an intensely enhancing lesion (arrow), compatible with intramuscular hemangioma. (Courtesy of Dr. Okwha Kim, South Korea.)
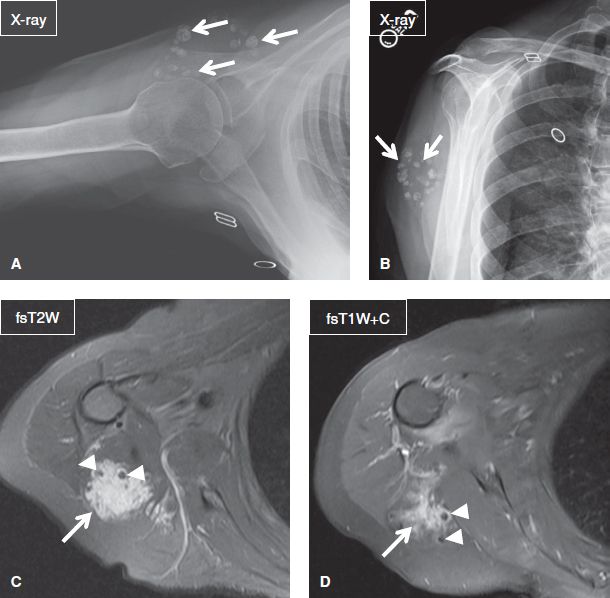
Fig. 3: Venous malformation in a 65-year-old woman. Axial view (A) and scapular Y view (B) radiographs of the right shoulder reveal multiple ovoid and punctuate calcifications (arrows) within the soft tissues of the posterior aspect of the shoulder. On the corresponding axial MR images (C, D), the lesion (arrows) appears well-defined, partially intramuscular and consists of multiple T2 hyperintense lobules including flow voids (arrowheads), and demonstrates serpiginous contrast enhancement.
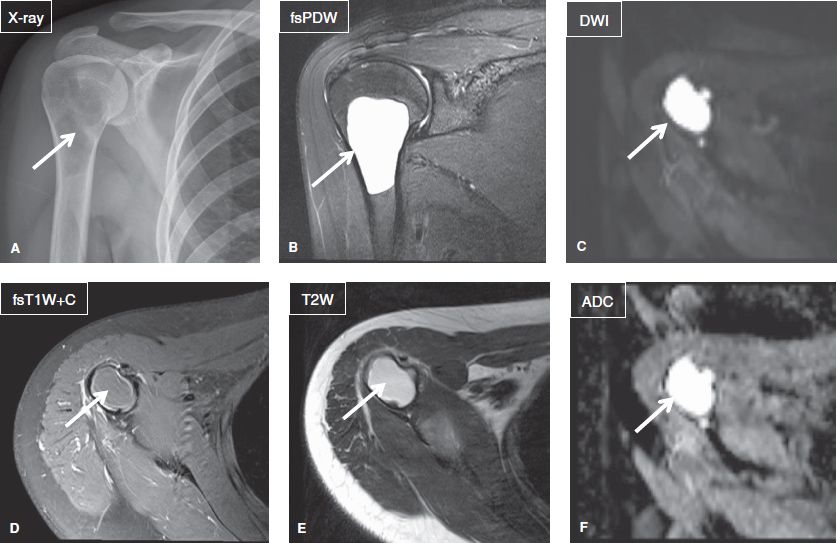
Fig. 4: Unicameral (simple) bone cyst in a 26-year-old woman. Anteroposterior radiograph (A) demonstrates a radiolucent lesion (arrow) with narrow zone of transition in the proximal humerus. On the corresponding coronal (B) and axial (D, E) MR images, the lesion (arrows) appears well defined, cystic, and nonenhancing. On quantitative imaging (C, F), the lesion (arrows) shows high ADC—2.5 × 10–3 mm2/s and increased signal on DWI due to T2 shine through, features, which indicate benignity.

Fig. 5: Avulsive cortical irregularity (cortical desmoid). Anteroposterior (A) and lateral (B) radiographs of the knee reveal a saucer-shaped radiolucent cortical irregularity (arrows) involving the posteromedial aspect of the distal femoral metaphysis. On the respective coronal (C), sagittal (D), and axial (E) MR images, the area of irregularity (arrows) is T2 hyperintense and corresponds to the attachment of the adductor magnus tendon. Cortical desmoid belongs to the skeletal “don’t touch” lesions.
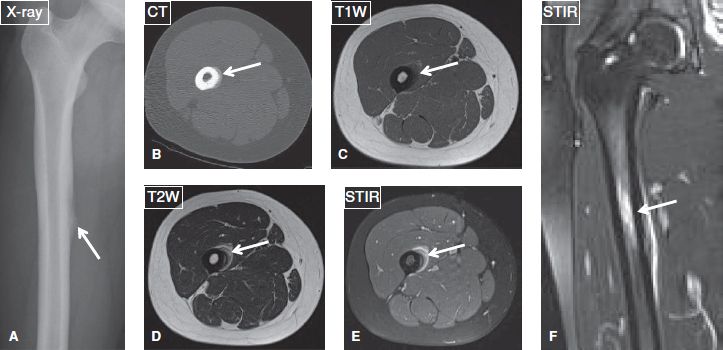
Fig. 6: Adductor insertion avulsion syndrome (thigh splint) in a 19-year-old woman ballet dancer, who presented with right thigh pain since 1 month. A: Anteroposterior radiograph shows focal periosteal reaction at the medial femoral shaft near the insertion of the adductor tendons (arrow). B: The periosteal reaction (arrow) is better delineated on the axial CT image. The respective axial (C–E) and coronal (F) MR images show linear hyperintensity and contrast enhancement (arrows), indicative of edema and hyperemia, respectively, along the medial aspect of the femoral shaft.
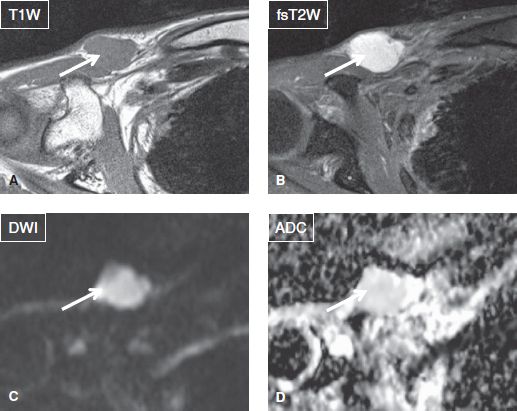
Fig. 7: Indeterminate lesion. Solid palpable mass in a 49-year-old female. Axial images demonstrate a well-defined mass (arrows) of homogeneous T1 isointense and homogeneous T2 hyperintense signal. Notice hyperintensity on DWI with high ADC value (1.8 × 10−3 mm2/s). Final biopsy diagnosis was well-differentiated myxoid liposarcoma.
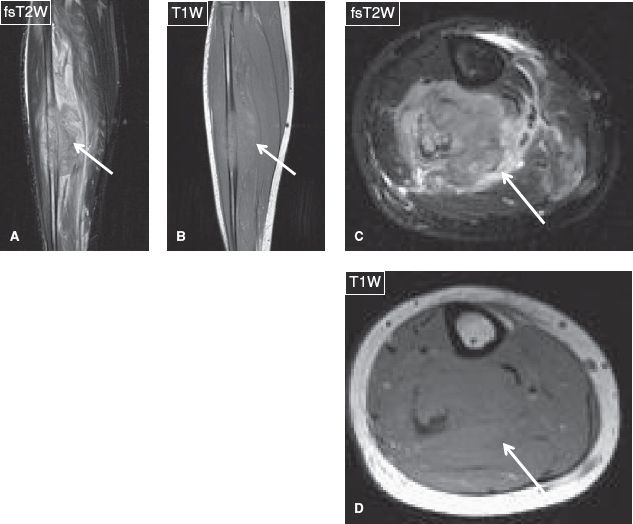
Fig. 8: Osteosarcoma. Coronal (A, B) and axial (C, D) images of the calf demonstrate an ill-defined mass (arrows) of marked heterogeneous signal and contrast enhancement, which emanates from the fibula and infiltrates the adjacent soft tissues.
 HOW TO FILL THE STRUCTURED REPORT
HOW TO FILL THE STRUCTURED REPORT
Markers have been [<placed> <not placed>] at the site of concern.
It is important that the technologist places markers on the painful and/or palpable bony or soft tissue findings. Thereby, if a large area is imaged, it becomes easier for the reader to identify the lesion, even if the latter is subtle or relatively obscure. This is particularly helpful if the lesion merely represents a palpable unencapsulated fat lobule or skin lesion.
TABLE 1: The MR imaging features, which assist in differentiating between malignant and benign musculoskeletal lesionsa
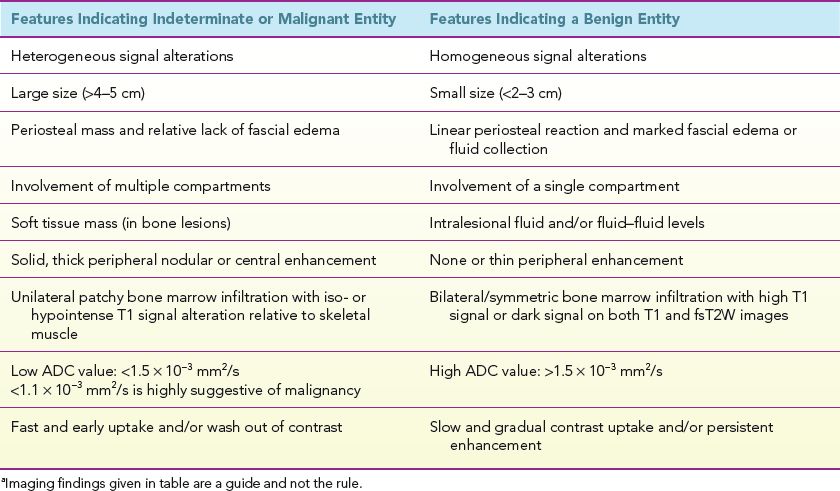
TABLE 2: Differential diagnosis of benign soft tissue lesion based on tissue and specific location characteristicsa
Size: [<>] × [<>] × [<>] cm
Generally, the larger the size of the lesion, the more are the chances that it is ominous or malignant (Fig. 9). A few exceptions to this rule include clear fat-containing lipoma, fibrolipomatous hypertrophy of the nerve, fluid-containing lesions, vascular malformations and fascial fibrous lesions, such as fibromatosis or desmoid (Figs. 10–12). Some benign lesions are associated with elongated bizarre-shaped lesions with or without cortical deformity and thickening, such as in fibrous dysplasia, neurofibromatosis, and Paget disease (Figs. 13–15). The above lesions have other characteristics that aid in the diagnosis such as young age, relative epiphyseal sparing unless associated with McCune Albright syndrome, cortical thickening and remodeling and mixed marrow signal changes and cystic changes with regions of T2 darkening in fibrous dysplasia; cutaneous stigmata, genetic markers, bony pseudoarthrosis, target and tail signs within the tumors and multiple NOFs in neurofibromatosis; predominant cortical/subcortical involvement and thickening with fibrofatty marrow changes, bone expansion and trabecular thickening, and predisposition among elderly Caucasian males in Paget disease.
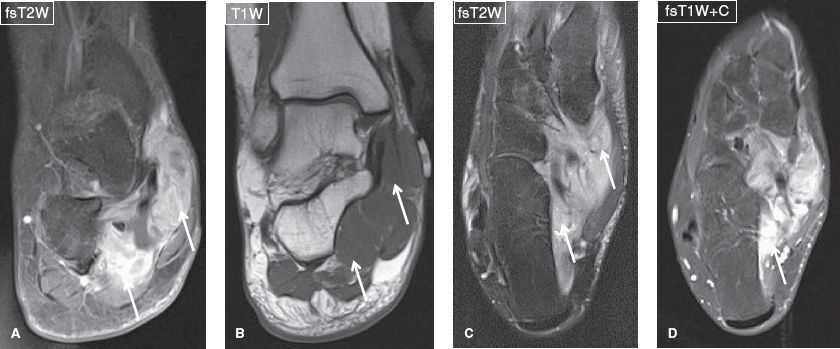
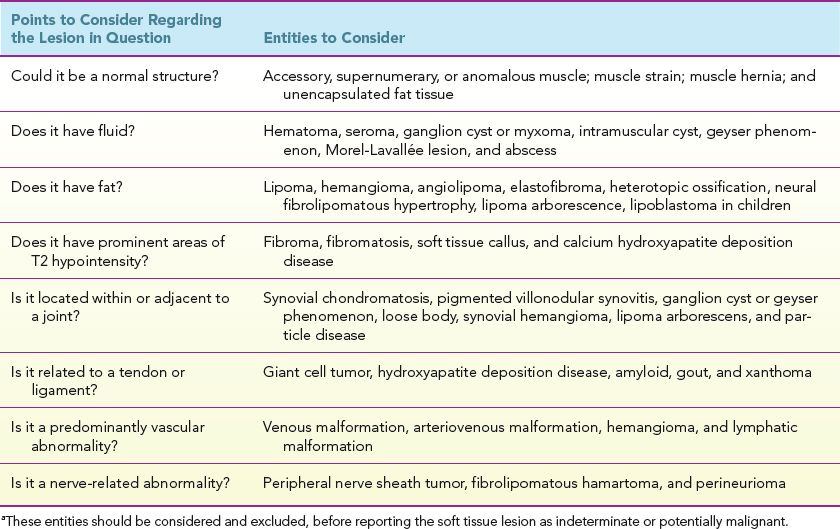
Fig. 9: Large mass: Synovial sarcoma. Coronal (A, B) and axial (C, D) images show a markedly enhancing T2 heterogeneous lesion (arrows) infiltrating the soft tissues of the medial aspect of the hindfoot and midfoot, including the tarsal tunnel.
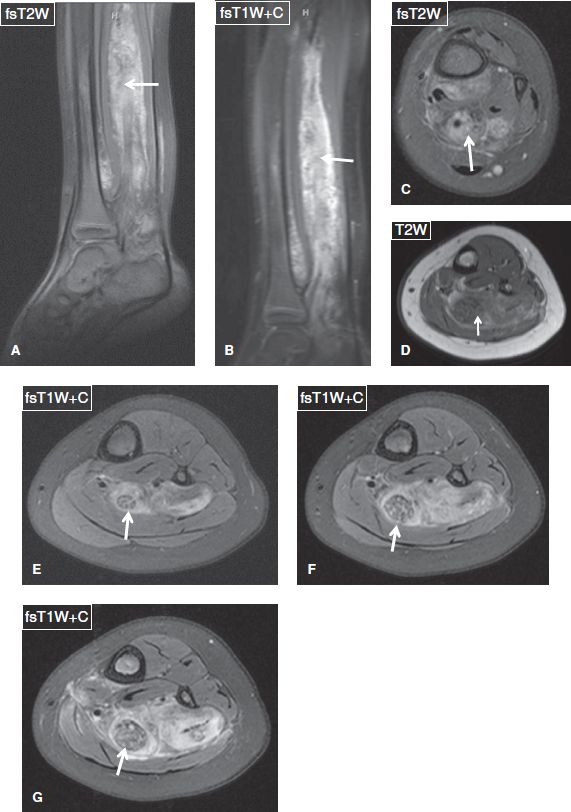
Fig. 10: Fibrolipomatous hamartoma (new name: lipomatosis of nerve, WHO 2013 classification): Noncontrast sagittal (A) and axial (C, D), and postcontrast sagittal (B) and axial (E–G) images show extensive fibrofatty hypertrophy of the tibial nerve (arrows) along with a vascular malformation in this otherwise benign developmental entity of fibrolipomatous hypertrophy. Notice coaxial cable appearance of the tibial nerve on the axial postcontrast images, classic for this entity.
Fig. 11: Whole-leg venous malformation in a 25-year-old man. Coronal (A, B) and axial (C, D) images show numerous dilated vessels (arrows) within the muscles and subcutaneous tissues of the lower extremity. E–G: Coronal images from time-resolved MR angiography using Ablavar show delayed filling of the dilated vessels in the venous phase (arrows) with no arterovenous shunting. H–I: The malformation (arrows) is depicted on delayed MR angiography images.
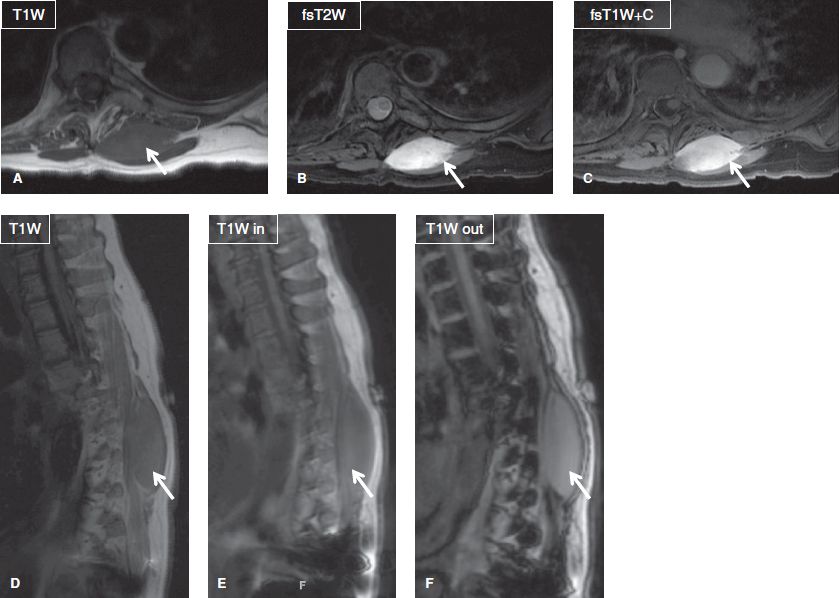
Fig. 12: Desmoid tumor in a 65-year-old woman. Axial (A–C) and sagittal (D–F) images exhibit a well-defined enhancing mass (arrows) of homogeneous intermediate T1 and high T2 signal within the paraspinal musculature. No loss of signal is seen within the lesion on out-of-phase images.
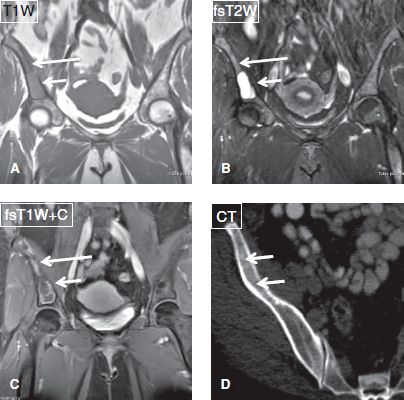
Fig. 13: Fibrous dysplasia in a 47-year-old woman. A–C: Coronal MR images show a lesion (long arrows) of intermediate T1 signal, mixed T2 signal, and peripheral enhancement involving the right iliac bone. A portion of the lesion (short arrows) is cystic. D: On axial CT scan, the lesion (arrows) features the typical ground-glass appearance of this entity.
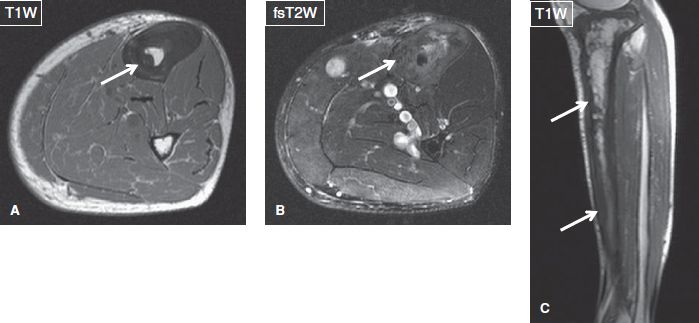
Fig. 14: Paget disease. Axial (A, B) and sagittal (C) images exhibit diffuse cortical thickening (arrows) and enlargement of the tibia with internal fibrofatty proliferation.
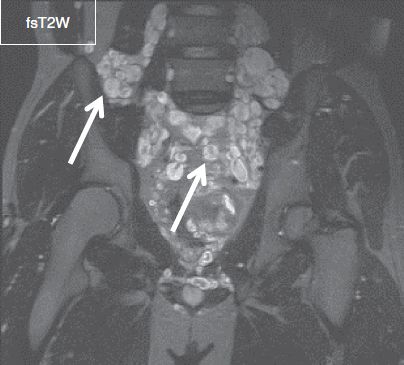
Fig. 15: Neurofibromatosis type I. Coronal image at the level of the pelvis demonstrates numerous ovoid T2 hyperintense lesions with target signs (arrows), which correspond to neurofibromas in this patient with extensive neurofibromatosis (“bag-of-worms” sign).
Location: [<>]
Location is very important for both bone and soft tissue lesions (e.g., malignancy almost never occurs within the joints with rare exceptions (Fig. 16), and in nearly all circumstances mass-like intra-articular lesions represent benign synovial processes) (Fig. 17).
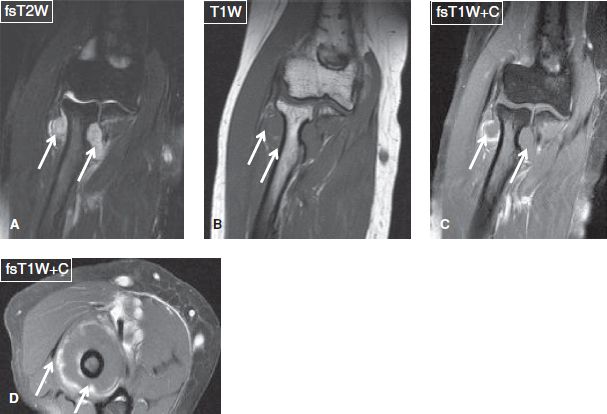
Fig. 16: Synovial chondrosarcoma in a middle-aged woman with a recent history of palpable mass around the right elbow. Coronal (A–C) and axial (D) images show lobulated mass (arrows) in the proximal radioulnar joint causing eccentric bony erosions and encircling the radius neck with peripheral nodular enhancement.
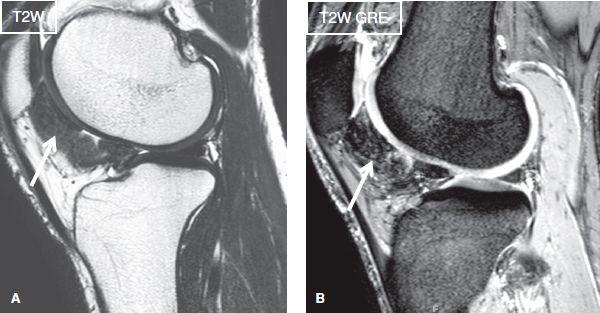
Fig. 17: Pigmented villonodular synovitis in a 45-year-old female. Sagittal images (A, B) show a hypointense amorphous lesion (arrows) at the posterior aspect of Hoffa fat pad, which corresponds to hemosiderin laden synovial mass. The signal is particularly evident on the gradient-echo image. Findings consistent with PVNS (new name: Tenosynovial giant cell tumor diffuse type, WHO 2013 classification).
Let’s discuss bony lesions first. Since metaphysis is the portion with the richest vascularity in long bones, most tumors start or eventually lodge in this location. Therefore, what could help the reader in the differential diagnosis would be the lesion epicenter preference in other areas. In children, lesions involving the epiphyses (or apophyses) include eosinophilic granuloma, subchondral cyst, and chondroblastoma. In adults, lesions involving the epiphyses include giant cell tumor (GCT, extending from the metaphysis after physeal fusion), clear cell chondrosarcoma, myeloma, metastasis, subchondral cyst (geode), and lipoma (Figs. 18–22). Lesions involving the diaphyses include osteoid osteoma, fibrous dysplasia, enchondroma, Ewing sarcoma, metastasis, myeloma, adamantinoma (in the tibia), lymphoma, and eosinophilic granuloma (mnemonic: O FEMALE) (Figs. 23, 24).
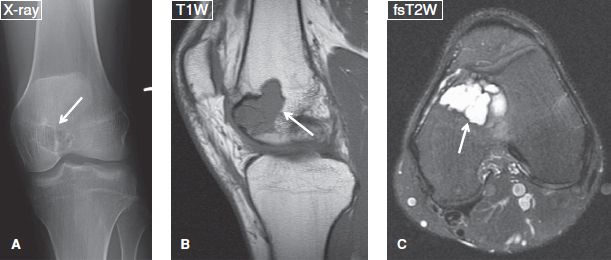
Fig. 18: Chondroblastoma. Anteroposterior radiograph (A) reveals a well-defined lytic lesion (arrow) with thin sclerotic margins at the femoral epiphysis. On the corresponding sagittal (B) and axial (C) MR images, the lesion (arrows) demonstrates lobulated margins and homogeneous fluid-like signal. Notice associated bone marrow edema, quiet common with chondroblastoma.
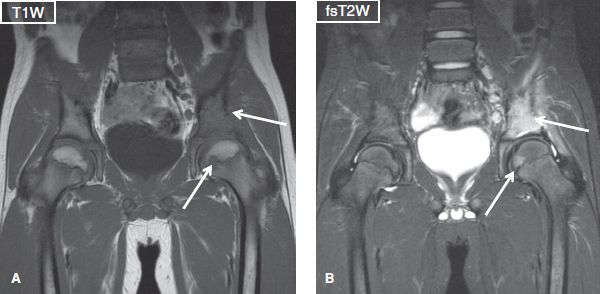
Fig. 19: Eosinophilic granuloma. Coronal images exhibit homogeneous T1 isointense/T2 hyperintense lesion (arrows) involving a large area of the left acetabular roof and an additional focus of the ipsilateral femoral head. Notice fascial edema in active stage of the disease, not an uncommon finding, and it can mimic infection.
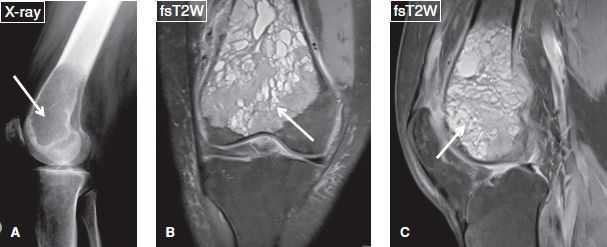
Fig. 20: Giant cell tumor in a 35-year-old woman. Lateral radiograph (A) of the knee displays a well-defined lytic lesion (arrow) without sclerotic margins at the distal femoral metaphysis extending into the epiphysis. The corresponding coronal (B) and sagittal (C) MR images reveal that the lesion (arrows) abuts the articular surface and appears heterogeneously T2 hyperintense to hypointense. Notice associated cortical permeation, not uncommon with this lesion.
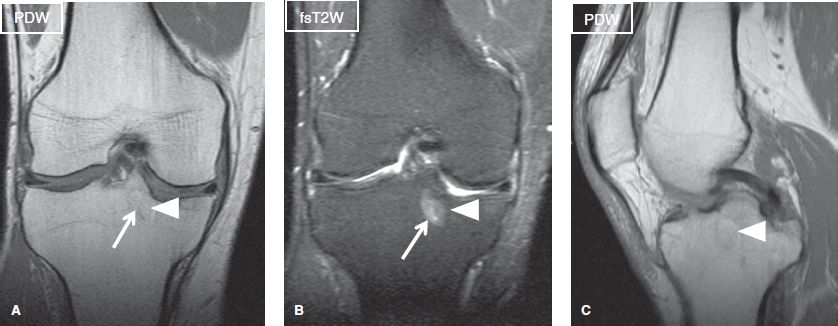
Fig. 21: Lipoma with cystic degeneration. Coronal (A, B) and sagittal (C) images demonstrate a well-defined lesion at the tibial epiphysis, which features partially fluid (arrows) and partially fat (arrowheads) signal.
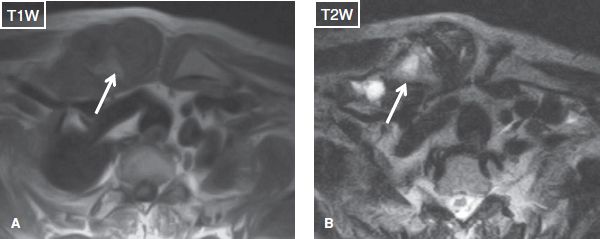
Fig. 22: Severe sternoclavicular joint osteoarthritis. Middle-aged patient presenting with palpable mass over the right sternoclavicular joint. Axial images exhibit significant capsular hypertrophy of the right sternoclavicular joint in the setting of severe osteoarthritis. Notice subchondral cysts in the right distal clavicle (arrows).
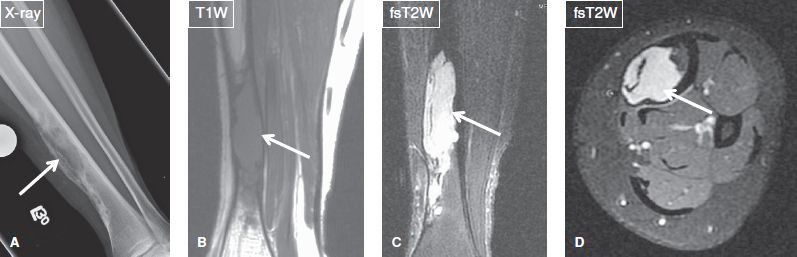
Fig. 23: Adamantinoma in a young woman. Anteroposterior radiograph (A) of the lower extremity demonstrates an aggressive lytic lesion (arrow) involving the distal tibial diaphysis. The corresponding coronal (B, C) and axial (D) MR images confirm the locally aggressive nature of the lesion (arrows), which appears solid, infiltrates the marrow and causes cortical erosion and bone enlargement.
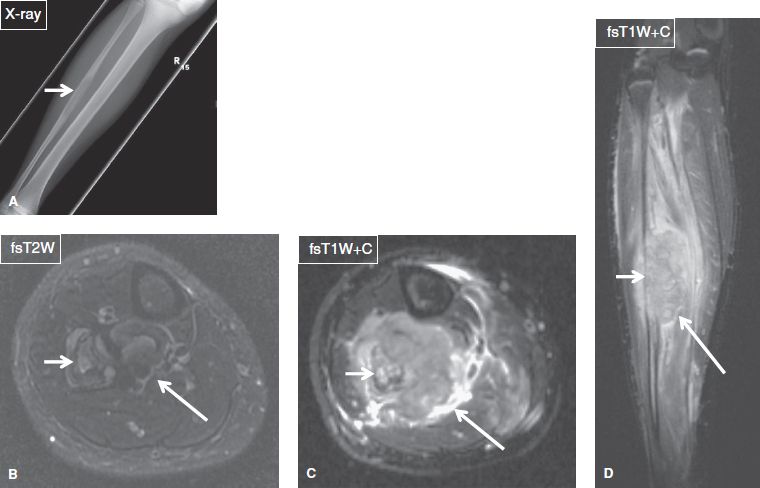
Fig. 24: Ewing sarcoma in a 12-year-old female. Anteroposterior radiograph (A) shows a lytic lesion (arrow) with wide zone of transition of the fibular diaphysis. Axial (B, C) and sagittal (D) MR images show a soft tissue mass (long arrows) of heterogeneous signal and contrast enhancement, which emanates from the (infiltrated) fibula (short arrows) and shows extracompartmental extension with encasement of the posterior tibial neurovascular bundle.
Lesions that classically and preferentially occur in the toes or fingers include Nora’s lesion, glomus tumor, epidermoid cyst, enchondroma, brown tumor, metastasis from lung cancer (Figs. 25–30). In the spine, most lesions occur in predictable locations: GCT, plasmacytoma, benign notochordal tumor, chordoma and clear cell chondrosarcoma mostly involve the vertebral bodies; chordoma in the lower sacrum or the C2 vertebra; osteoid osteoma, osteoblastoma, and metastases in the pedicles; aneurysmal bone cyst (ABC) and chondrosarcoma in the posterior elements; and peripheral nerve sheath tumors and perineural cysts in and around the neural foramina (Figs. 31–41). Multiple posterior element involvement may be seen with chondrosarcoma, ABC, and tuberculosis (Fig. 42). A limited number of lesions can cross the joint capsule, include GCT, ABC, chondrosarcoma, and plasmacytoma. Finally, synovial sarcoma rarely arises in the joint, but it commonly occurs in para-articular locations.
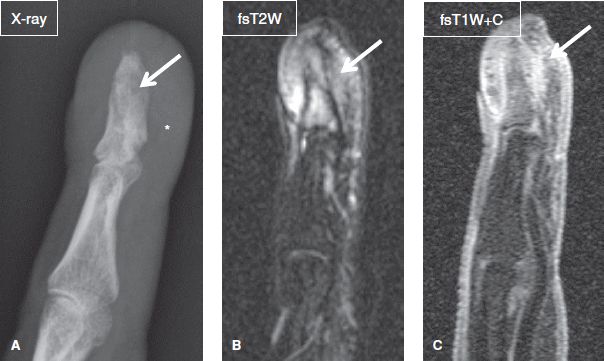
Fig. 25: Nora lesion (bizarre periosteal osteochondromatous proliferation, BPOP) of finger. A: Lateral radiograph of the index finger shows aberrant periosteal and cortical thickening (arrow) of the distal phalanx as well as swelling of the surrounding soft tissues (asterisk). B, C: The respective sagittal MR images exhibit intensely enhancing T2 hyperintense subcutaneous tissues (arrows) at the distal phalanx, associated with marrow edema and enhancement.
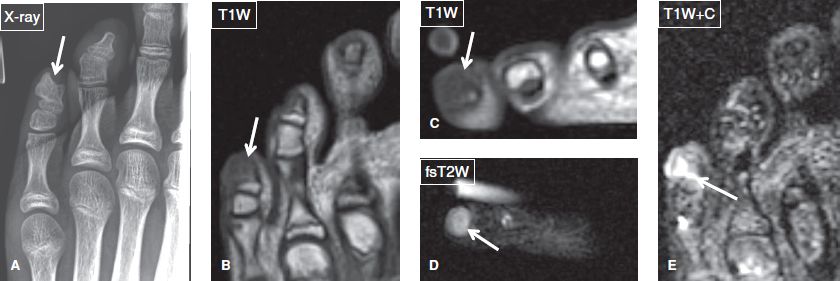
Fig. 26: Nora lesion (bizarre parosteal osteochondromatous proliferation) of little toe. Anteroposterior radiograph (A) of the forefoot shows a well-defined osseous proliferation (arrow) at the tip of the distal phalanx of the fifth toe. On the respective coronal (B), axial noncontrast (C, D), and coronal (E) postcontrast MR images, the lesion (arrows) shows intermediate T1 and high T2 signal with soft tissue and bone marrow edema and enhancement.
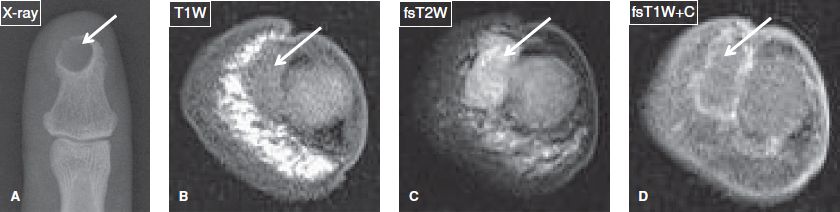
Fig. 27: Epidermoid cyst. A: Anteroposterior radiograph of the thumb demonstrates a well-defined lytic lesion (arrow) with narrow zone of transition at the tip of the distal phalanx. B–D: On the corresponding axial MR images, the lesion (arrows) shows fluid-like signal and thin peripheral enhancement.

Fig. 28: Glomus tumor. Anteroposterior radiograph (A) demonstrates mild focal erosion (arrow) of the distal phalanx of the finger with soft tissue swelling. The respective axial (B) and coronal (C) MR images reveal a small ovoid intensely enhancing lesion (arrows) of high T2 signal, located between the nail and the distal phalanx.
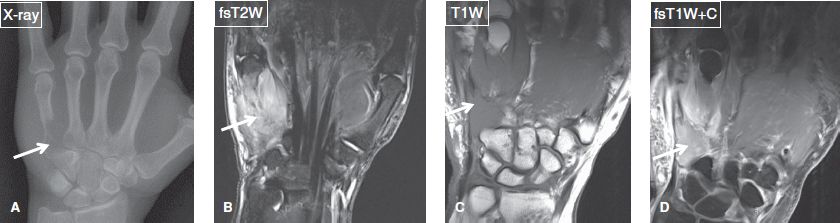
Fig. 29: Metastasis to the hand from lung cancer. A: Anteroposterior radiograph of the hand reveals extensive osteolysis (arrow) at the proximal half of the fifth metacarpal bone. B–D: The corresponding coronal MR images show an intensely enhancing ill-defined soft tissue mass (arrows) arising from metastasis to the fifth metacarpal bone.
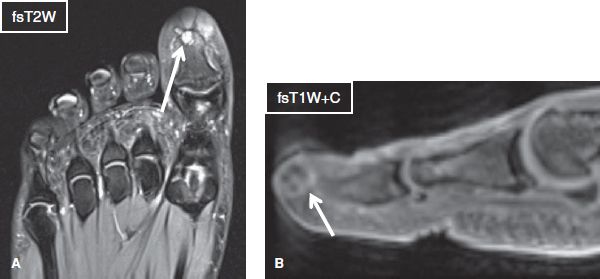
Fig. 30: Bone metastasis in a 30-year-old woman with history of malignancy. Axial (A) and sagittal (B) images of the forefoot exhibit a well-defined T2 hyperintense lesion (arrows) at the tip of the distal phalanx of the first toe, which demonstrate mild, mostly peripheral contrast enhancement. Biopsy proved metastatic tumor from lung carcinoma.
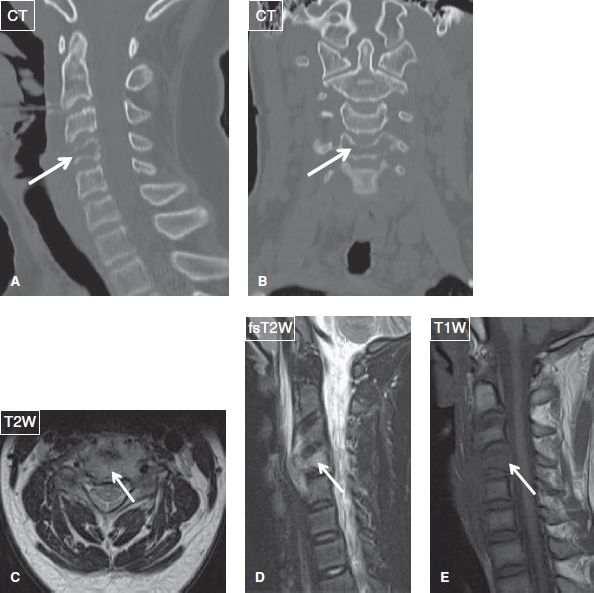
Fig. 31: Eosinophilic granuloma (Langerhans cell histiocytosis). Sagittal (A) and coronal (B) reformatted CT images demonstrate osteolytic lesion and compression fracture of the C4 vertebral body (arrows). On the respective axial (C) and sagittal (D, E) MR images, T2 hyperintense and T1 isointense mass (arrows) erodes the C4 vertebral body and spreads to the prevertebral space.
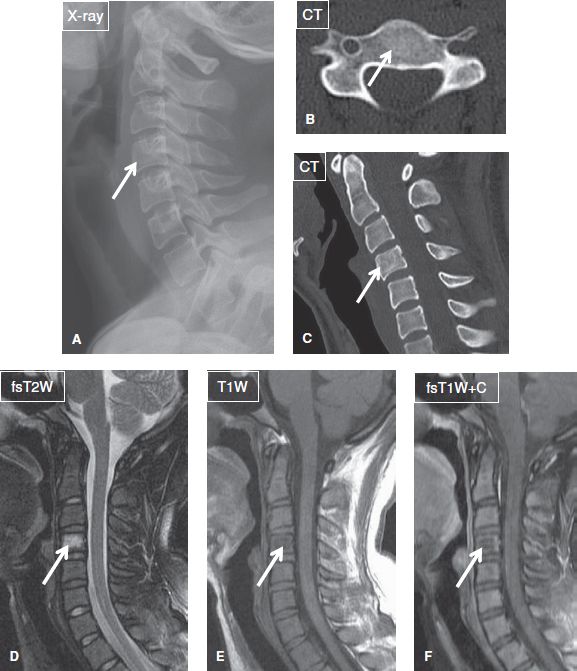
Fig. 32: Benign notochordal cell tumor in a young woman. A: An indistinct ovoid lesion (arrow) with thin sclerotic margins is seen in the C4 vertebral body on lateral radiograph of the cervical spine. Axial (B) and sagittal (C) reformats from a CT study reveal an ill-defined lesion with internal sclerosis (arrows). D–F: On the corresponding sagittal MR images, the lesion (arrows) shows relatively low T1/high T2 signal and no appreciable contrast enhancement.
Fig. 33: Small chordoma in an old woman. Axial (A–C) and sagittal (D) images demonstrate a T1 isointense, T2 hyperintense, and heterogeneously enhancing mass (arrows) eroding the lower sacrum and coccyx.
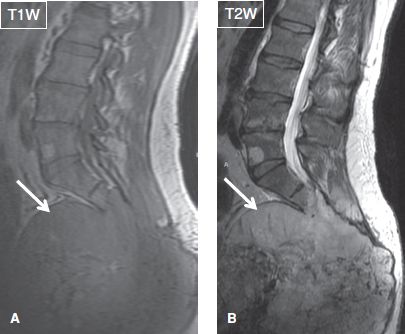
Fig. 34: Large chordoma in a middle-aged man. Sagittal images of the lumbosacral region exhibit a large and heterogeneous mass (arrows) emanating from the sacrum and coccyx. Notice incidental hemangioma in L5 vertebra.
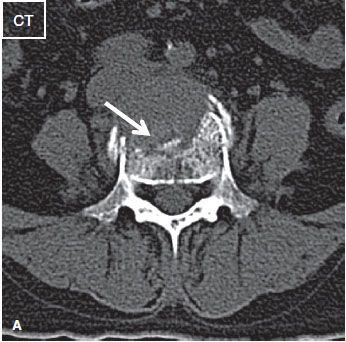
Fig. 35: Multiple myeloma in a middle-aged woman with several month history of low back pain. A: Axial CT image shows erosion (arrows) of the anterior aspect of the L4 vertebral body with a soft tissue mass. No sclerosis or internal mineralization seen.
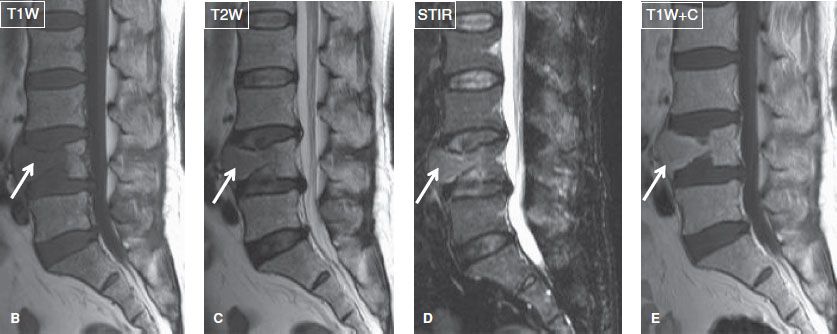
Fig. 35: B–E: On the corresponding sagittal MR images, there is a compression fracture of the L4 vertebral body, the anterior aspect of which is infiltrated by homogeneous tissue (arrows) of intermediate T1/relatively high T2 signal and moderate contrast enhancement.
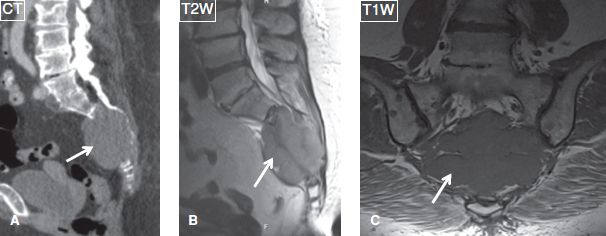
Fig. 36: Plasmacytoma. A: Sagittal reformat from a CT study demonstrate an isodense mass (arrows) eroding the sacrum with epicenter in the sacral body. B, C: The lesion (arrows) features intermediate T1 and minimally increased T2 signal intensity.
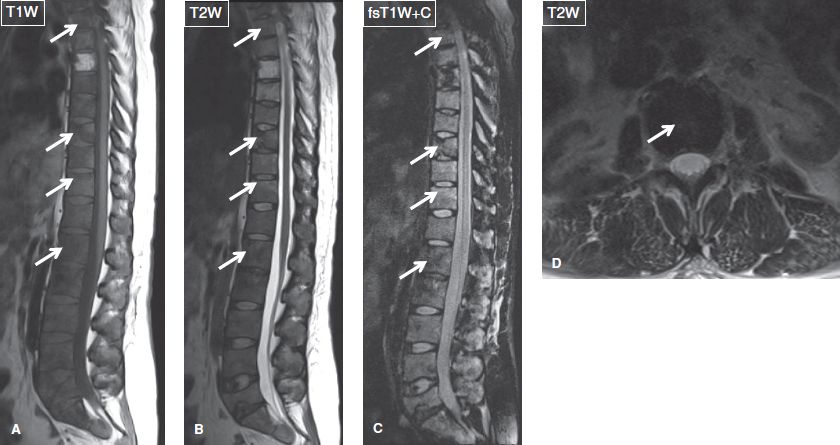
Fig. 37: Breast metastases. Sagittal (A–C) and axial (D) images of the thoracic and lumbar spine demonstrate numerous hypointense, enhancing lesions (arrows) diffusely infiltrating the vertebrae, which correspond to sclerotic metastatic foci. Notice L5 vertebral collapse with diffuse marrow infiltration and pot belly anterior margin in keeping with a pathologic compression fracture.
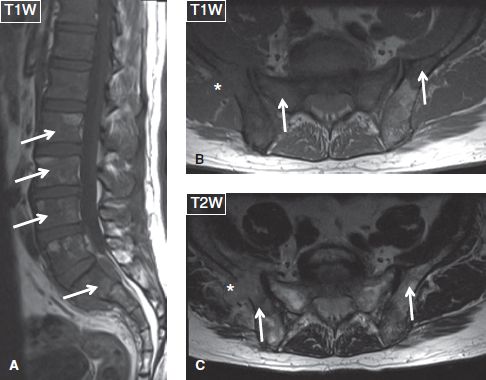
Fig. 38: Lymphoma. Sagittal (A) and axial (B, C) images exhibit multiple T1 hypointense/T2 hyperintense lesions (arrows) at the spine, sacrum, and iliac bones, one of which (asterisk) features extraosseous extension.
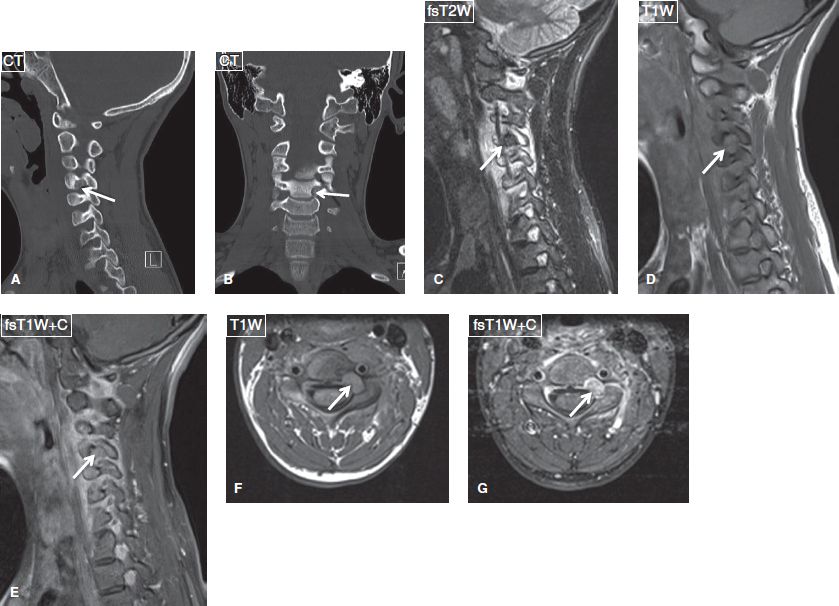
Fig. 39: Osteoid osteoma. Sagittal (A) and coronal (B) reformatted CT images demonstrate focal lytic lesion with internal mineralization and peripheral sclerosis of the left C4 pedicle (arrows). On the respective sagittal (C–E) and axial (F, G) MR images, the lesion (arrows) features intermediate T1/T2 signal and intense contrast enhancement and is associated with edema of the adjacent bone marrow and soft tissues.
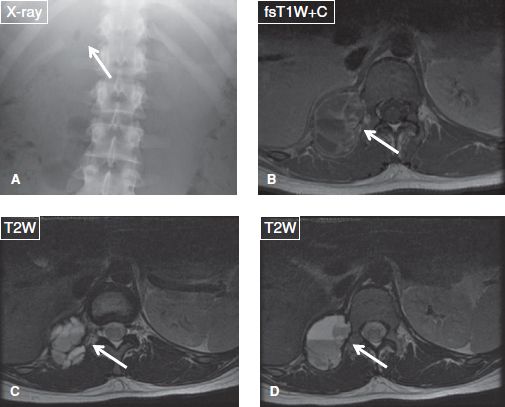
Fig. 40: Aneurysmal bone cyst. A: Anteroposterior radiograph shows osteolysis of the right twelfth rib and erosion of the adjacent posterior elements of T12 vertebra (arrow). B–D: The corresponding axial MR images demonstrate a well-defined multiloculated lesion (arrows), featuring fluid signal and fluid–fluid levels. The lesion shows peripheral and internal septal enhancement, typical of ABC.
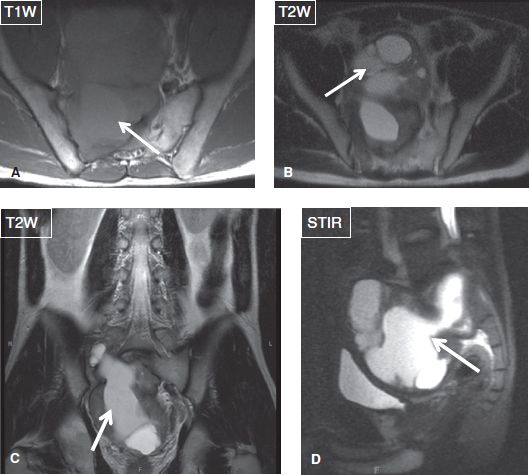
Fig. 41: Cystic schwannoma in a young man. Axial (A, B), coronal (C), and sagittal (D) images show a large mass (arrows), which emanates from the right sacral neural foramina, projects in the pelvic cavity, and features cystic and hemorrhagic components.
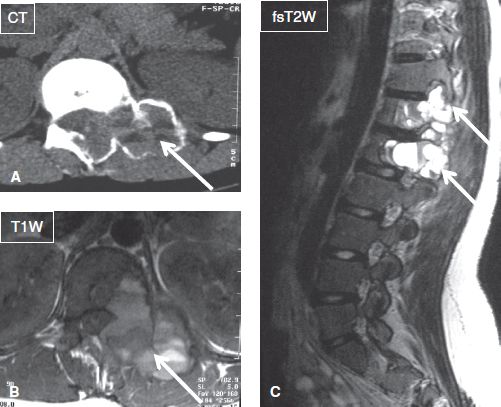
Fig. 42: ABC. Axial CT image (A) along with axial (B) and sagittal (C) MR images shows an expansile osteolytic lesion with fluid–fluid levels (arrows) involving the T12 and L1 vertebrae in continuity.
Among soft tissue tumors, location is also very important from diagnostic perspective apart from internal characteristics. Soft tissue lesions can be accurately diagnosed merely based on location. Intra-articular bodies or cysts are encountered in or near a joint and include ganglion, parameniscal, paralabral, pericruciate, geyser phenomenon, various bursal lesions around the knee, postoperative or injury-related seroma, and Morel-Lavallée (i.e., degloving lesion from injury) (Figs. 43–48). Lesions developing within skeletal muscles include intramuscular cyst, parasitic infestation, myxoma, lipoma, elastofibroma dorsi, venous malformation, endometriosis, and myositis ossificans/heterotopic ossification (Figs. 49–53). Lesions developing in tendons, fasciae, and ligaments include calcium hydroxyapatite disease, gout, GCT of tendon sheath, amyloidosis, xanthoma, fibroma in relation to plantar fascia, juvenile aponeurotic fibroma, nodular fasciitis, myositis ossificans, fibromatosis, desmoid tumor, and dermatofibrosarcoma protuberance in the skin and subcutis. Elastofibroma dorsi typically develops in the periscapular and gluteal areas (Fig. 50). The most common soft tissue lesions arising in the foot include intermetatarsal bursitis (along the dorsum of the toes), Morton neuroma and foreign body granuloma (along the plantar aspect of the toes), adventitial bursitis (at pressure points), and tophi or granulomatous nodules from rheumatoid arthritis and sarcoidosis (Figs. 54–61). Finally, lesions developing along the transverse axis of long bones may be characterized as follows.
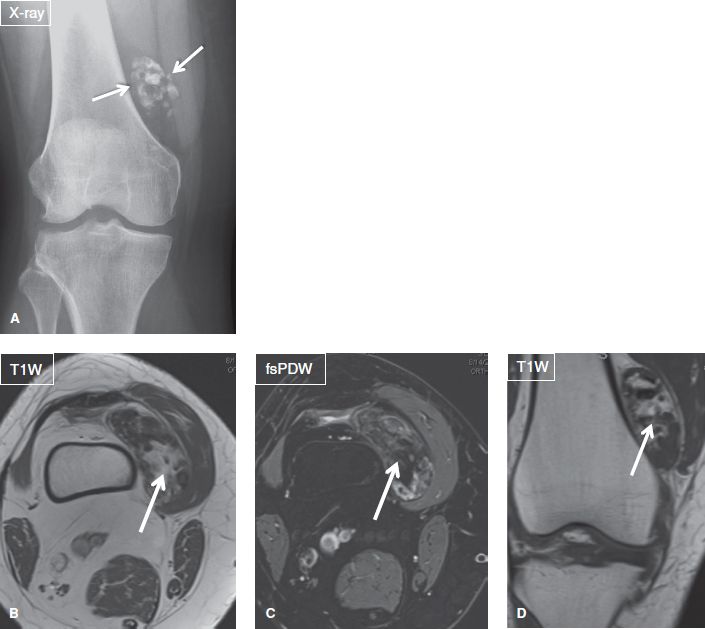
Fig. 43: Intra-articular body in a middle-aged woman who presented with knee pain. Anteroposterior (A) radiograph reveals a cluster of coarse calcifications (arrows) in the region of suprapatellar pouch. Notice underlying moderate degenerative changes. The respective axial (B, C) and coronal (D) MR images show a heterogeneous mass-like lesion within the suprapatellar bursa, a large osteochondral body.
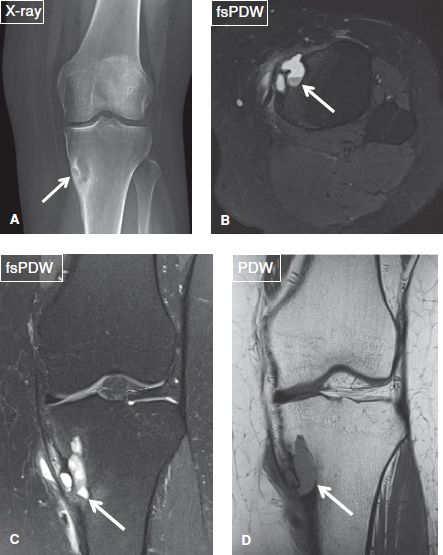
Fig. 44: Cortical avulsion cystic change. Anteroposterior radiograph (A) of the knee shows an radiolucent lesion at the tibial metaphysis with sclerotic margin. On the respective axial (B) and coronal (C, D) MR images, the lesion (arrows) appears cystic with fluid level, is located at the pes anserinus insertion, and is associated with overlying cortical discontinuity. Findings are consistent with avulsive cystic change.
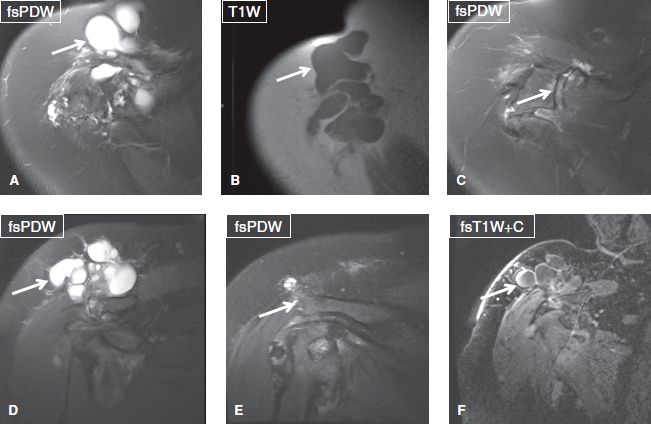
Fig. 45: Geyser phenomenon in a 59-year-old woman who presented with focal swelling at the level of the acromioclavicular joint. Axial (A–C) and coronal (D–F) images of the right shoulder exhibit a multiloculated cystic lesion (arrows in A, B, D, F) superior to and abutting the acromioclavicular joint and os acromiale synchondrosis, which show degenerative changes (arrows in C, E). There was peripheral enhancement on postcontrast images. Underlying rotator cuff was deficient. Findings consistent with geyser phenomenon, a ganglion that communicates with the shoulder joint and develops along the path of least resistance, usually from AC joint. In this case, it also extended from the os acromiale synchondrosis (arrow in E).
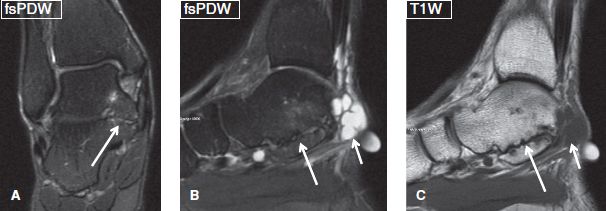
Fig. 46: Ganglion cyst from coalition pseudoarthrosis. Coronal (A) and sagittal (B, C) MR images show middle and posterior facet talocalcaneal fibrous coalition at the ankle (long arrows). Notice the ganglion cyst (short arrows) arising from the posterior aspect of the coalition, presenting as a palpable mass.

Fig. 47: Morel-Lavallée lesion in a 18-year-old man. Axial (A) and sagittal (B, C) images of the left knee exhibit a heterogeneous hematoma, developed between the subcutaneous fat and the superficial fascia, as a result of traumatic separation of the fascial layers.
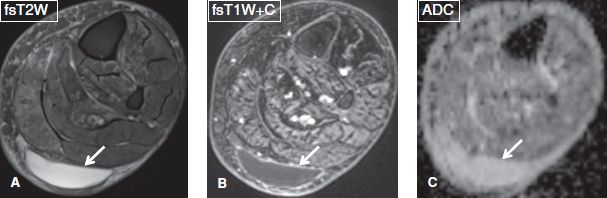
Fig. 48: Seroma. Axial images. A, B: A smoothly marginated lesion (arrows) is evident between the muscles and the subcutaneous tissues of the posterior superficial compartment, which features homogeneous high T2 signal and thin peripheral enhancement, in keeping with a postoperative seroma. C: The high ADC value (2.4 × 10–3 mm2/s) of the cystic lesion (arrow) confirms its cystic nature.
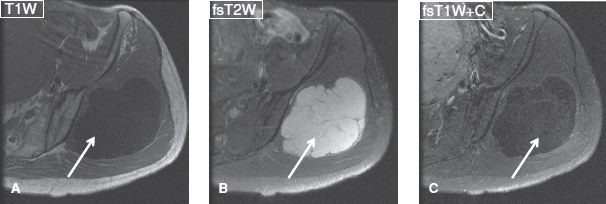
Fig. 49: Myxoma. Axial images through the pelvis demonstrate a well-defined multiloculated cystic lesion (arrows) in the gluteal muscles with cystic appearance and mild patchy internal enhancement on the postcontrast subtraction image (C), a classic site and imaging appearance of intramuscular myxoma.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


