Chapter 23 Biomechanics of the foot
Nomenclature
The terms pronation and supination represent a combination of movements of the foot. When the foot is pronated, there is dorsiflexion of the ankle, eversion of the subtalar joint, and abduction of the transverse tarsal joint. When the foot is supinated, there is plantarflexion of the ankle joint, inversion of the subtalar joint, and adduction of the transverse tarsal joint.
Walking cycle
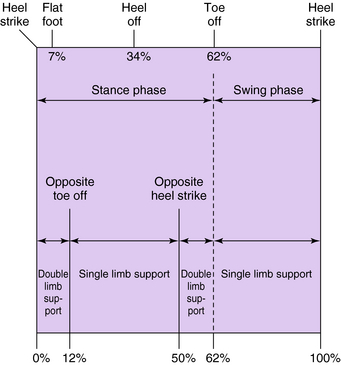
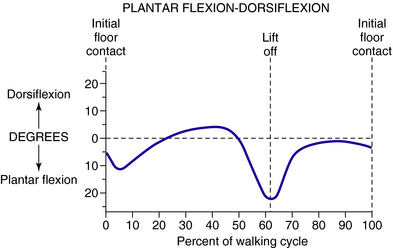
The walking cycle describes the repetitive nature of gait. By convention it begins and ends with heel strike of the same foot. The walking cycle is divided into a stance phase, in which the foot is on the ground, and a swing phase, in which the foot is off the ground and swinging forward. Normally, stance phase consumes approximately 60% of the walking cycle and swing phase 40% (Fig. 23-1). The stance phase is further divided into two periods of double-limb support and one period of single-limb support. The initial period of double-limb support begins with initial ground contact and ends with toe-off of the opposite limb at 12% of the cycle. Single-limb support then occurs until 50% of the cycle, when the opposite foot strikes the ground, entering the second period of double-limb support. This is shortly followed by lift-off at 62% of the cycle, which initiates the swing phase.
Weight-bearing forces
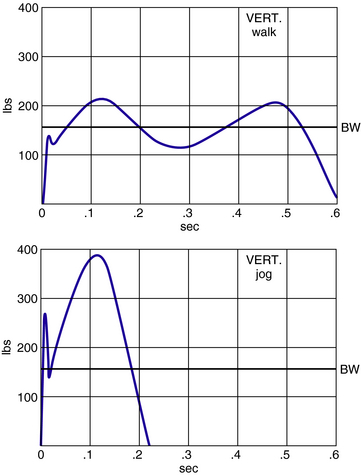
As we walk, equal and opposite forces are created at the interface between the foot and the ground. One way to measure these forces is a force plate, which consists of load cells applied in orthogonal directions to a suspended platform. In this way, the overall vertical force, fore and aft shear, and medial–lateral shear can be directly measured during the gait cycle. At heel strike, the initial impact against the ground creates a vertical force of approximately 80% of body weight (Fig. 23-2). This rapidly rises to an initial peak of approximately 115% of body weight, representing the transfer of weight to the stance foot at opposite side toe-off. During this initial peak the body’s center of gravity is accelerating upward in a sinusoidal pattern as the body moves over the extended leg. As the center of gravity reverses direction, there is a relative unloading of the foot and a corresponding dip in the vertical force curve to approximately 80% of body weight. A second peak of about 110% of body weight occurs when the heel rises and weight moves over the metatarsal heads. This counteracts the downward motion of the body’s center of gravity. The vertical force against the ground rapidly falls after opposite heel strike. It reaches zero at the time of toe lift-off, indicating that the toes are lifted from the floor rather than forcefully push off the floor. The magnitude of the force against the ground can vary. A person walking slowly exerts less force than when walking quickly and much less than when jogging or running.
Measuring plantar pressures on discrete points of the foot can be accomplished using a variety of devices. The Harris mat and optical pedobarograph largely have been supplanted by arrays of miniature pressure transducers, which have superior temporal, spatial, and measurement resolution. These arrays can be built into a shoe insert or arranged as a grid on the floor, so they can be used in a variety of in vitro and in vivo studies. In this way, the pressures experienced by discrete points on the foot can be analyzed during gait. This type of study reveals a large initial force against the heel, which rapidly passes from the heel to the metatarsal area (Fig. 23-3). The foot usually is on the ground for approximately 620 ms. By approximately 300 ms all of the force is concentrated in the metatarsal region, after which it is transferred distally to the toes, particularly the hallux.

Anatomical basis of foot and ankle biomechanics
Ankle joint
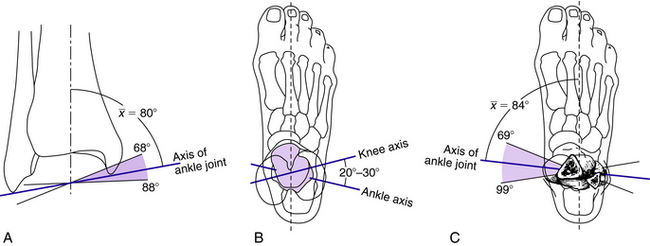
The axis of the ankle joint passes just distal to the tip of each malleolus and can be estimated by placing one finger on each malleolus. Anthropometric studies demonstrate that although the tibial plafond is parallel to the floor, the angle between the axis of the ankle joint and that of the long axis of the tibia is tilted medially about 80 degrees (Fig. 23-4).6 Comparing the long axis of the foot with the ankle axis, the foot is slightly internally rotated. In relation to the axis of the knee, the ankle axis is externally rotated approximately 20 to 30 degrees. These axes vary slightly from person to person, so when carrying out an ankle arthrodesis it imperative that the rotation of the operated extremity match that of the opposite side.
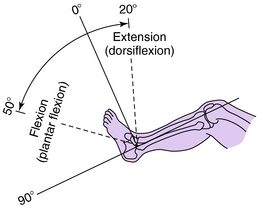
The motion that occurs at the ankle joint is that of dorsiflexion and plantarflexion. Dorsiflexion is most accurately assessed when the calcaneus is placed in line with the tibia and the head of the talus is covered by the navicular. This places the foot in neutral position (Fig. 23-5). Passively, dorsiflexion is approximately 20 degrees and plantarflexion 50 degrees, although a great deal of variation exists among individuals. Figure 23-6 shows the normal rotation that occurs at the ankle joint during walking.
Subtalar joint
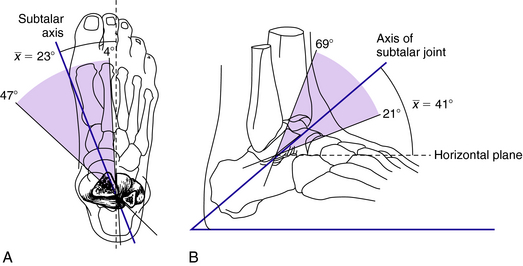
The axis of rotation of the subtalar joint is oblique to both the sagittal and transverse planes. In the transverse plane, it deviates approximately 23 degrees medially from the long axis of the foot. In the sagittal plane, it deviates approximately 40 degrees superiorly to the horizontal plane (Fig. 23-7).1,7 There is a significant degree of variation in the axis of the subtalar joint from individual to individual.
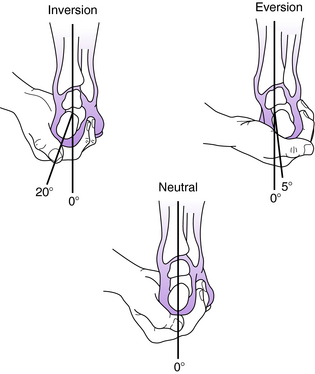
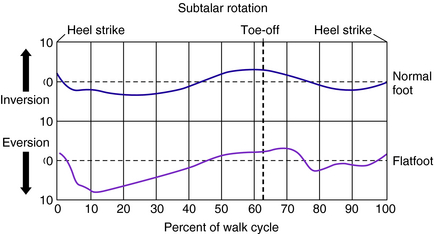
The motion that occurs in the subtalar joint is that of inversion and eversion. Inversion is movement of the heel in an inward direction, and eversion is movement outward (Fig. 23-8). The range of motion of the subtalar joint includes inversion of approximately 30 degrees and eversion about 10 degrees, although there is significant variation from individual to individual. During normal walking, eversion occurs at the time of initial ground contact until about 15% of the stance phase, after which progressive inversion occurs until the time of toe-off. The magnitude of eversion during the stance phase is about 8 degrees in individuals with a normal foot and 12 degrees in individuals with flat foot (Fig. 23-9).16 In individuals with a cavus foot, the degree of subtalar motion is less than that observed in normal feet.
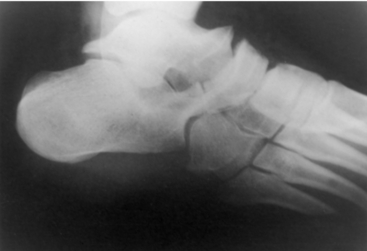
Inman6 believed that the axis of the subtalar joint permitted it to function as an oblique hinge-type mechanism. This oblique hinge mechanism permits rotatory motion to be passed back and forth between the lower extremity and foot (Fig. 23-10). Specifically, transverse plane rotation in the tibia is linked distally with hindfoot eversion/inversion and farther distally into transverse tarsal joint rotation (forefoot varus/valgus). Normal function of the subtalar joint requires normal function of the talonavicular and calcaneocuboid joints. If normal motion cannot occur in either of these joints, the motion in the subtalar joint is significantly restricted. Similarly, when subtalar joint motion cannot occur, increased stress is placed on the ankle joint proximally and the talonavicular joint distally. When subtalar stiffness is long-standing, degenerative arthrosis or a ball-and-socket ankle joint may result (Fig. 23-11), and changes in the talonavicular joint may occur (Fig. 23-12).
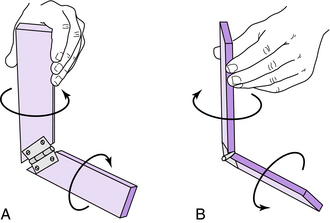

Transverse tarsal joint
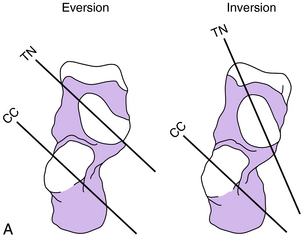
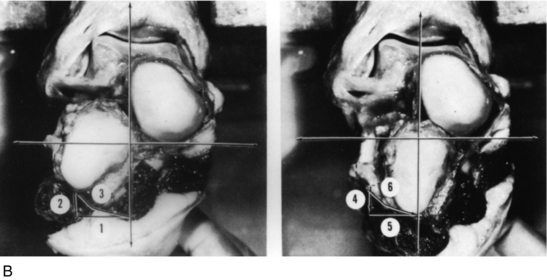
The transverse tarsal joint consists of the talonavicular and calcaneocuboid joints. The transverse tarsal joint should be considered an integral part of the subtalar joint, because for normal motion to occur in the transverse tarsal and subtalar joints all three joints must function in a normal manner. The transverse tarsal joint motion has been studied by Elftman,3 who demonstrated that when the axes of the talonavicular and calcaneocuboid joints are parallel to one another, there is flexibility in the transverse tarsal joint, but when the axes are nonparallel, there is rigidity (Fig. 23-13). When the subtalar joint is in an everted position, the transverse tarsal joint axes are parallel, and the transverse tarsal joint is flexible. This is the observation at the time of initial ground contact (heel strike) when impact absorption is desirable. In the last half of the stance phase, a progressive inversion occurs in the subtalar joint, which results in the axes becoming nonparallel. This results in rigidity of the transverse tarsal joint and allows the forefoot to act as a rigid lever.
< div class='tao-gold-member'>

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


