Chapter 9D Autologous Chondrocyte Implantation
Transarthroscopic Implantation of Hyalograft (Hyaff 11) with Autologous Chondrocytes
Introduction
It has been demonstrated to be an optimal physical support to allow cell-cell contacts, cluster formation, and extracellular matrix deposition and to deliver differentiated chondrocytes.1,2
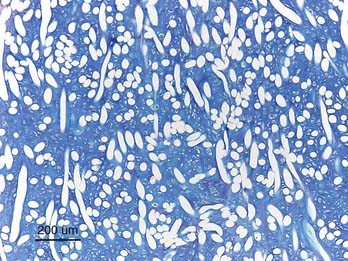
The cells harvested from the patient are expanded and then seeded onto the scaffold where the cells are able to redifferentiate and retain a chondrocytic phenotype even after a long period of in vitro expansion in monolayer culture1,2 (Fig. 9D-1). The Hyalograft with cultured chondrocytes may be implanted by press fitting directly into the lesion as described by Kon et al.3 The scaffold has self-adhesive properties, but most often additional fibrin glue is needed for a secure positioning. In this chapter, the authors describe a modified implantation technique: the “folded blanket” technique for the knee and for the ankle.
Technical Overview
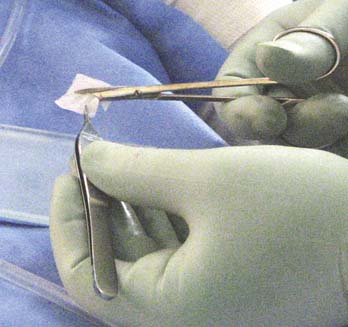
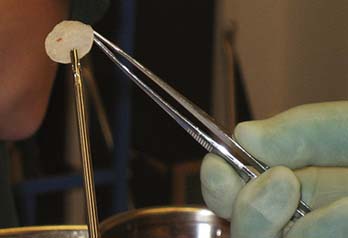
Cartilage is harvested as described in Chapter 9C. The cell culture takes a longer time to grow compared to when cells are transplanted as suspension. After 4 to 5 weeks, the scaffold is delivered as 2 × 2 cm large patches (Fig. 9D-2). Depending on the quality of the cultured cells, the seeded scaffolds have different strength.
Operative Technique for the Knee
A half pipe introducer may be used to introduce the scaffold into the joint.
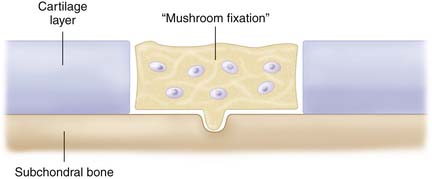
The defect has already been debrided as described in Chapter 3. The central part of the defect is treated by a microfracture awl to get a fixation point (mushroom fixation) (Fig. 9D-3).
The chondrocyte-seeded matrix is then cut with a scissor or scalpel to the approximate size of the defect (Fig. 9D-4).
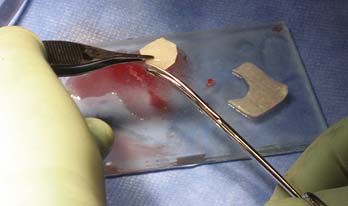
FIGURE 9D-4 The chondrocyte-seeded matrix is cut with a scissor or scalpel to the approximate size of the defect.
The scaffold is covered with a thin fibrin glue layer (Fig. 9D-5), grasped with an arthroscopic grasp instrument with plain surfaces (Fig. 9D-6), and introduced into the joint along the half pipe intruder to reach the defect (Fig. 9D-7).

FIGURE 9D-5 The scaffold is covered with a thin layer of fibrin glue and becomes saturated and easier to handle.

Some extra fibrin glue is injected over the implanted scaffold, and the scaffold is compressed toward the defect bottom with a curved smooth tonsil elevator. If the scaffold is oversized, the edges may be folded like a blanket into the defect to fill it up entirely (Fig. 9D-8).
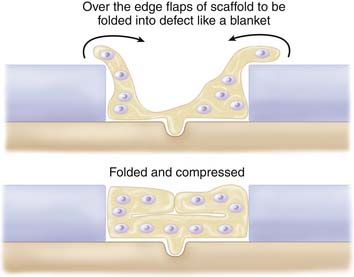
FIGURE 9D-8 If the scaffold is oversized, the edges may be folded like a blanket into the defect to fill it up entirely.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


