the 2.7-mm and the 4-mm wide angles. In the great toe joint and other tarsal joints, the 2- to 2.7-mm systems are the most appropriate.
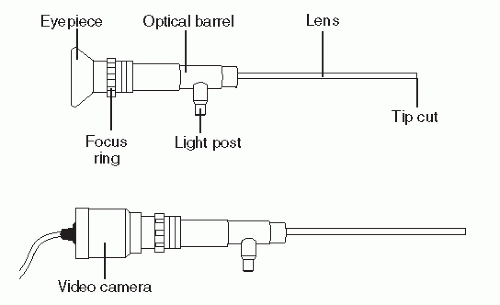 Figure 53.1 The anatomy of the arthroscope. |
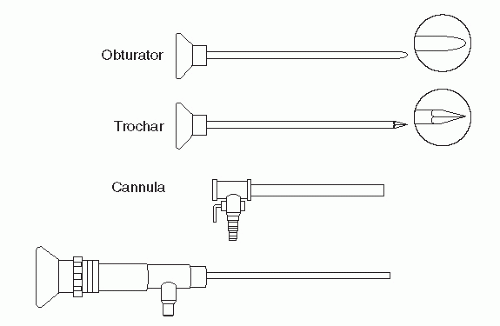 Figure 53.2 Instruments used to introduce the arthroscope into the joint. |
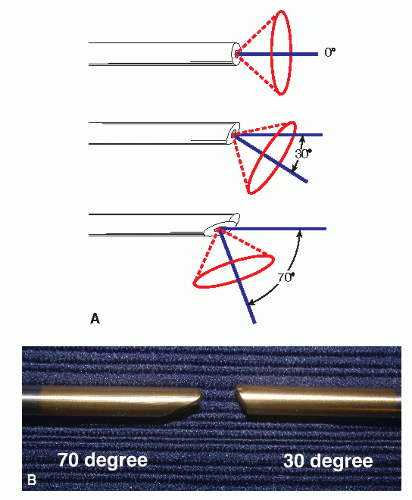 Figure 53.3 A: Effect of tip cut of various types of arthroscopes. B: Close-up comparison of 30- and 70-degree tip cuts. |
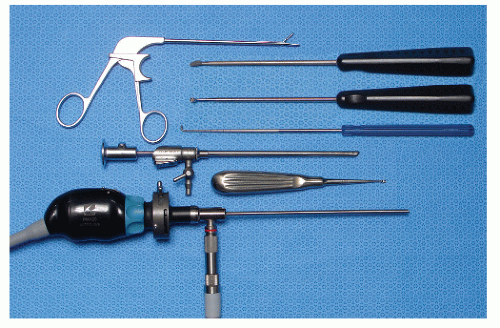 Figure 53.4 Appearance of a typical Mayo stand setup for foot and ankle arthroscopy. |
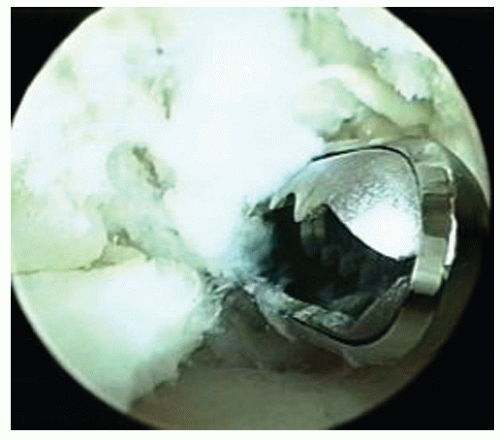 Figure 53.5 A 3.5-mm motorized arthroscopic shaver. |
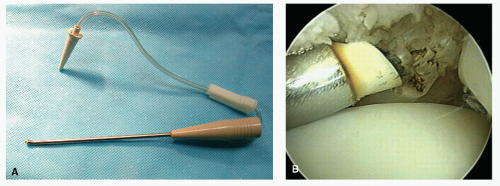 Figure 53.6 A: Example of a bipolar radiofrequency wand. Note 50-degree angle at tip and aspirated system. B: Bipolar wand being used to ablate anterolateral impingement. |
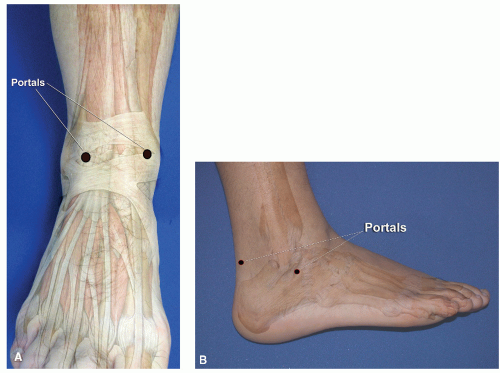 Figure 53.7 A: Topographical anatomy pertaining to portal placement for anterior ankle arthroscopy. B: Topographical anatomy for subtalar arthroscopy. |
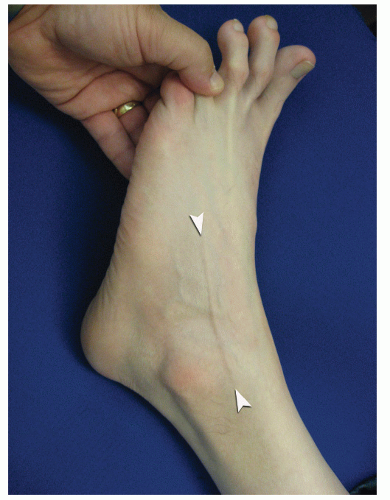 Figure 53.8 Passive plantarflexion of foot and fourth toe causing bow stringing (between arrowheads) of the IDCN. |
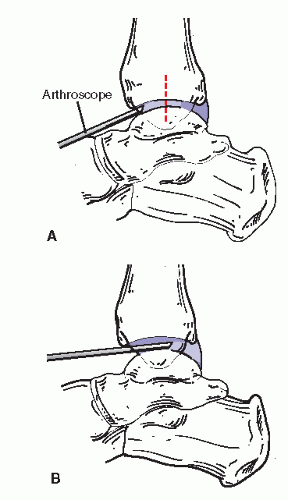 Figure 53.9 Diagram illustrating arthroscope access across the talar dome in undistracted joint (A) and distracted joint (B). Note how the scope orientation changes as it passes posterior. |
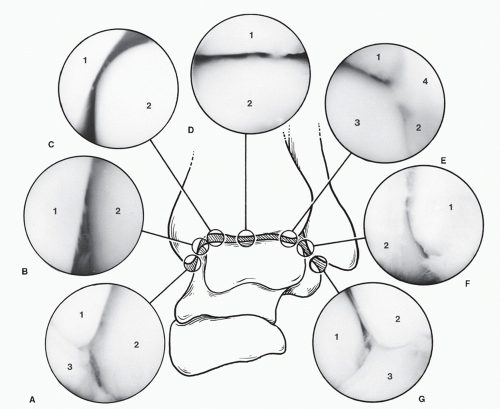 Figure 53.10 Normal arthroscopic intra-articular anatomy of the anterior aspect of the ankle. A: Deltoid ligament and inferior aspect medial malleolus, talus (1, tip of medial malleolus; 2, talus; 3, deltoid ligament). B: Talar medial malleolar joint (1, medial malleolus; 2, talus). C: Medial shoulder to talotibial joint (1, tibia; 2, medial shoulder of talus). D: Tibiotalar joint (1, tibia; 2, talus). E: Tibiofibular-talar articulation (1, tibial; 2, fibula; 3, lateral shoulder of talus; 4, tibiofibular synovial fringe). F: Talofibular joint (1, lateral malleolus; 2, talus). G: Anterior talofibular ligament and inferior aspect of lateral malleolus, talus (1, talus; 2, tip of lateral malleolus; 3, anterior talofibular ligament). |
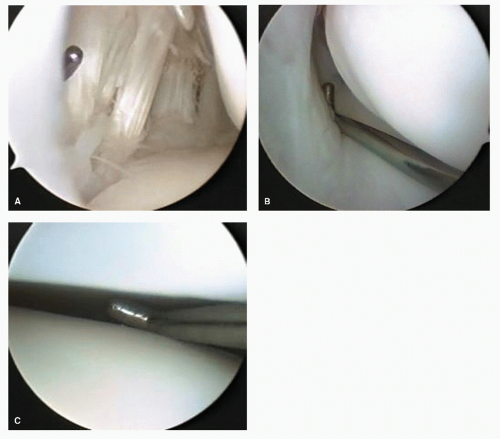 Figure 53.11 Arthroscopic images of the normal subtalar joint anatomy. A: Anterior capsule and retinacular elements of sinus tarsi. B: Interosseous ligament. C: Posterior facet. |
which additional leg stabilization or leg elevation off the operating table surface is necessary (Fig. 53.12). However, in the vast majority of cases, simple padding, straps, and sand bags offer sufficient positioning assistance and immobilization.
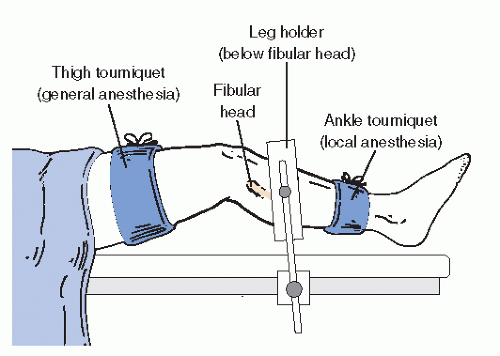 Figure 53.12 Illustration of one type of positioning and support of the leg with tourniquet positioning options. |
joint is either invasive (employing a device that directly engages bone) or noninvasive (using straps or bands) to pull the articular structures apart physically. Devices vary significantly in complexity, cost, and efficacy. A simple noninvasive distraction involves using bandages affixed to the foot, then applying distal traction either by attaching them to weights or to the surgeon himself, who then leans backward from the ankle (27,28). Commercially available noninvasive distraction systems employing mechanical distractors fastened to the operating table, then applied to a padded clove hitch strap binding the hindfoot, are available and have a proven record of safety in the adult patient (Fig. 53.13). Countertraction for most noninvasive methods is very helpful. A urologic knee stirrup placed in the popliteal fossa is often helpful in providing countertraction. As with scenarios involving positioning a patient, serious care of subcutaneous neurovascular structures are necessary to prevent complications.
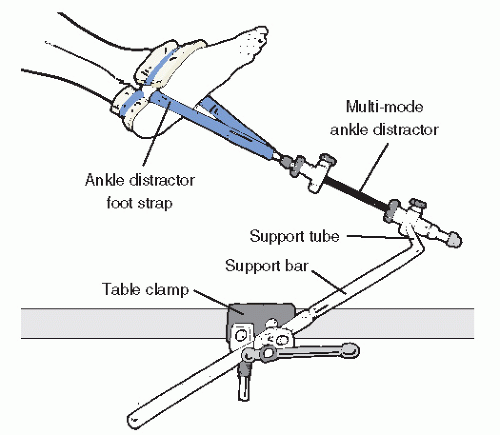 Figure 53.13 Illustration of joint noninvasive joint distraction setup. |
TABLE 53.1 Common Foot and Ankle Arthroscopic Portals | ||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
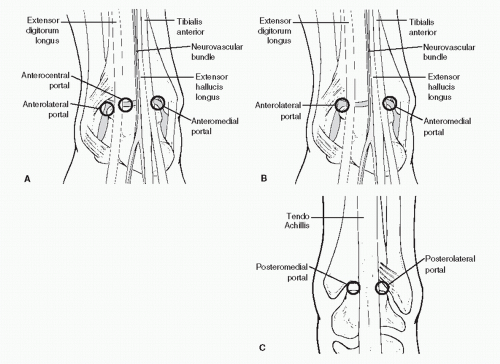 Figure 53.14 Classic portals of the anterior and posterior ankle. A: Anterior three-portal technique. B: Anterior two-portal technique. C: Posterior portal placement. |
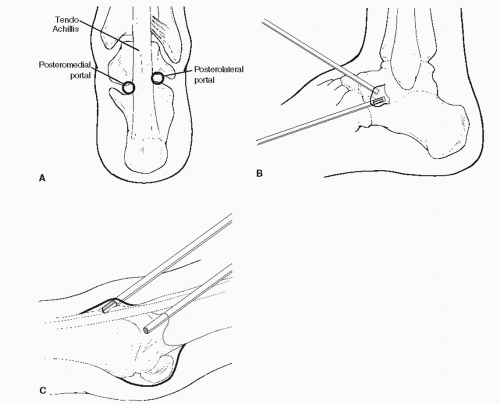 Figure 53.15 Classic portals of the subtalar and great toe joints. A: Posterior subtalar portals. B: Anterior approaches to the subtalar joint. C: First MTPJ portals. |
extra-articular (nonresponsive) or within the joint. A symptom complex that does not respond at least temporarily to an intraarticular injection of local anesthetic with or without steroid will not likely benefit from arthroscopy or other surgical maneuvers. Congenital bands and plicas can be found in the ankle and can cause localized symptoms usually coupled with an increase in activities (Fig. 53.17).
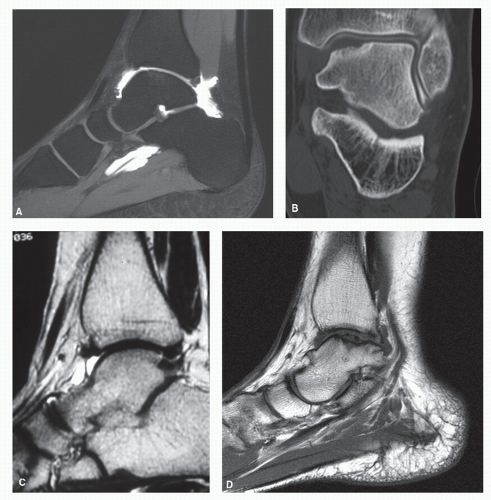 Figure 53.16 Diagnostic images: (A) MRI gadolinium arthrogram sagittal STIR image that shows continuity between the ankle and subtalar joints and the flexor hallucis longus tendon sheath. Note how the study allows enhanced visualization of the cartilage surface with partial thickness cartilage ankle joint defects on the anterior tibial and talar surfaces. B: CT arthrogram after arthroscopic excision of osteochondral fracture fragment. Note fibrocartilage filling of lesion site as highlighted by joint contrast agent. C: MRI arthrogram, sagittal slice on a T1-weighted image highlights intra-articular adhesion in the anterior joint recess. D: MRI demonstrating large osteochondral defect or talus. |
white over time (Fig. 53.18B). This hypertrophic tissue can occupy a large portion of the capsular reflection. Hypertrophic synovitis, whether chronic, acute, or mixed, sometimes fills the anterior pouch completely. In some situations, the reactive tissue becomes adherent to the juxta-articular bone and capsule. This condition is sometimes termed adhesive capsulitis because the tissue tends to contract, ultimately limiting movement and becoming impinged at the anterior joint line. Resection of adhesive capsulitis is frequently necessary to visualize the joint and define or discover the primary lesion, if it is still present.
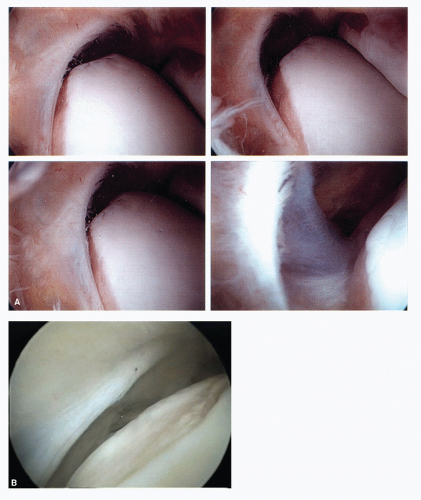 Figure 53.17 A: Anterior lateral ankle capsule with congenital band showing interaction with anterior talar body in different ankle positions. B: An example of a linear-oriented congenital band causing talar dome erosion. Note these bands are localized thickenings of the joint capsule and are covered by synovium. |
meniscoid lesions, impingement lesions, and adhesions are all similar lesions that are characterized as well-defined fibrocartilaginous bodies attached to periarticular structures, occasionally to bone and cartilage (Fig. 53.19) (46,47,48 and 49).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


