CHAPTER 17 Arthroscopic Treatment of Elbow Fractures
TREATMENT
Indications and Contraindications
Arthroscopic management of elbow fractures is a rapidly evolving indication for the use of elbow arthroscopy in the identification and treatment of intra-articular pathology. The technique provides for a minimally invasive surgical exposure, minimizing further soft tissue trauma in a region notorious for wound complications. Arthroscopic débridement of fibrinous and osseous debris facilitates postoperative elbow range of motion. Visualization of fracture fragments and chondral injuries is often superior to that achieved with open approaches, and it minimizes the requirements for intraoperative fluoroscopy. Identification of intra-articular pathology not evident on preoperative imaging enables appropriate treatment measures and a more accurate prognosis. Elbow arthroscopy can be used in combination with indirect reduction techniques to maximize articular congruity, or it can be used for direct arthroscopic reduction with fixation devices passed into the joint.
Conservative Management
Most intra-articular fractures of the distal humerus can be effectively treated with open reduction and internal fixation (ORIF), and superior results are achieved with this approach compared with skeletal traction or cast immobilization. Khalfayan and colleagues1 concluded that patients with displaced Mason type II radial head fractures who were treated conservatively had more pain, decreased strength, and decreased elbow motion compared with patients treated with open osteosynthesis. Radial head fracture treatment depends on the fracture pattern and displacement and includes early mobilization, ORIF, and resection or prosthetic replacement. Open treatment options for displaced olecranon fractures include tension band wiring, lag screw placement, neutralization plating, and excision with extensor mechanism reconstruction. Capitellar fractures can likewise be excised or stabilized with standard open techniques. Cadaveric research has drawn attention to the important stabilizing role of the coronoid and has provided compelling evidence for surgical management of these fractures in various circumstances.2,3
Arthroscopic Technique
The patient is placed prone or in the lateral decubitus position. The lateral decubitus position typically requires a supportive device to provide arm suspension. With the patient in the prone position, the arm is elevated on a 4-inch padded block with the elbow flexed to 90 degrees over an arm board located at the patient’s side parallel to the table (Fig. 17-1). This method avoids compression of neurovascular structures in the axilla and facilitates medial or lateral access (in case an open procedure becomes necessary) by internal or external rotation of the forearm onto the arm board. The forearm and hand should be wrapped with compressive wrapping material to restrict swelling and fluid extravasation. Intravenous prophylactic antibiotics are routinely administered preoperatively.

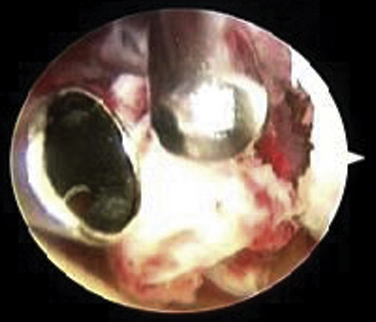
Most procedures can be accomplished with the 4.0-mm, 30-degree arthroscopic camera. A 70-degree camera can provide visualization of the capitellum or radial head from a posterior portal when instrumentation is required from the soft spot portal. Graspers with teeth and smooth outer surfaces are preferred to prevent hang-up on soft tissue. A 3.5-mm, full-radius arthroscopic shaver is useful for removal of organized fracture hematoma and debris (Fig. 17-2). Various implants can be used for fixation, contingent on the fracture configuration (discussed later).
After fracture stabilization has been achieved, the surgeon should thoroughly evaluate elbow stability. This can be accomplished with the assistance of fluoroscopy, but it can also be readily assessed arthroscopically. Diagnosis and management of associated ligamentous injuries of the elbow are discussed in Chapters 13 and 14.
Radial Head Fractures
Radial head fractures are the most common type of elbow fracture in adults, and they offer an excellent opportunity for arthroscopic evaluation and management (Fig. 17-3A). In patients with persistent locking and pain despite radiographic evidence of minimally displaced radial head fractures, diagnostic arthroscopy enables accurate assessment of articular cartilage, identification of any osteochondral flaps or loose bodies, and débridement with minimal morbidity. Displaced two-part radial head fractures can be visualized through a proximal anteromedial or posterolateral portal to assess the degree of articular incongruity, fracture fragment stability, and any impingement to forearm rotation. A direct lateral portal can also provide visualization of the posterior aspect of the radial head during confirmation of fracture reduction. If arthroscopic reduction with internal fixation is desired, visualization is best achieved with a 70-degree camera from a posterolateral portal, with instruments and implants introduced through a soft spot portal.
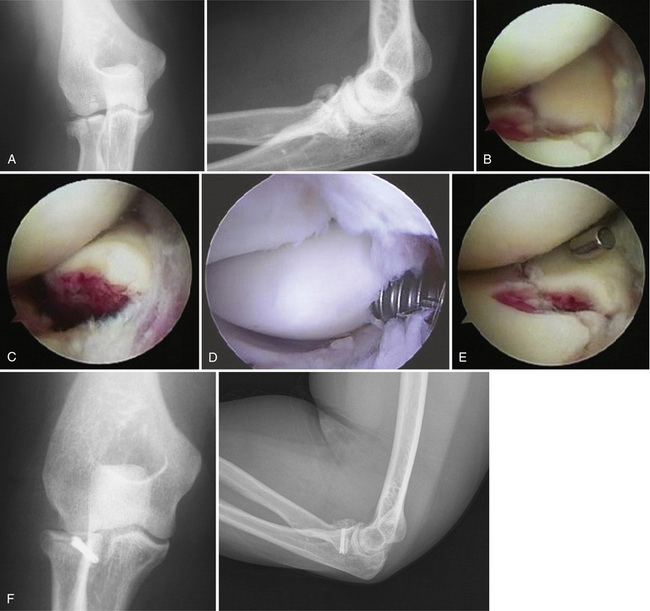
After débridement and lavage, Kirschner wires can be positioned through the anterolateral or soft spot portals in conjunction with arthroscopic probes, graspers, and occasionally, a reduction tenaculum to allow for manipulation, reduction, and provisional fixation of larger fracture fragments. Visualization can often be facilitated by rotating the forearm into maximal supination. Definitive fixation can then be performed using absorbable pins or cannulated screws (see Fig. 17-3D). Herbert-Whipple screws (Zimmer, Inc., Warsaw, IN) and headless variable-pitch screws (Acutrak screws, Acumed, LLC, Hillsboro, OR) are advantageous in providing secure fixation with compression to allow early motion, while being buried beneath the articular surface to avoid impingement. Reduction and stability of the fixation can be directly assessed during full rotation of the elbow (see Fig. 17-3E).
Rolla and colleagues4 reported preliminary results for six patients who underwent arthroscopic reduction and internal fixation for radial head fractures classified as Mason5

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


