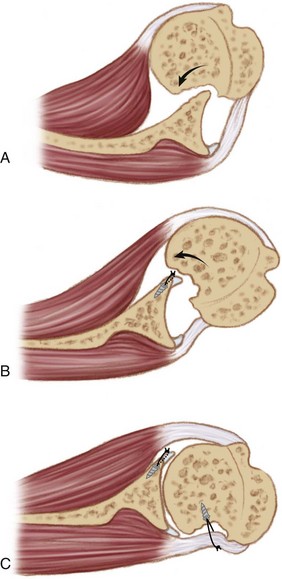
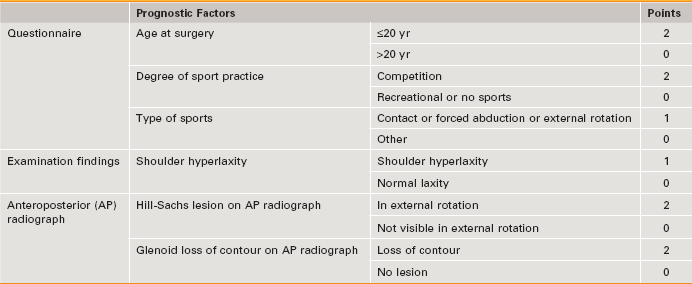
Chapter 17 • Indications: Anterior shoulder instability with associated large Hill-Sachs defects as visualized on preoperative plain radiographs, computed tomography (CT) scanning, or magnetic resonance imaging (MRI) or identified as engaging the glenoid surface during diagnostic arthroscopy at the time of instability surgery. • Contraindications: Isolated glenoid bone loss; other forms of shoulder instability than that in an isolated traumatic anterior direction. • Surgical technique: AHSR is not indicated as an isolated procedure. It is always performed in combination with an anterior capsulolabral repair. • Adequate preoperative workup is important to fully assess the size and location of osseous deficiency on both the humeral and glenoid sides of the shoulder joint. • An accessory posterolateral portal is established through which the base of the lesion is debrided and suture anchors are inserted. • The anterior repair must be prepared before proceeding to the posterior procedure, as the working space within the joint is significantly reduced after remplissage. • Once the humeral sutures have been placed, repositioning of the arthroscope in the posterior subdeltoid space before knot tying is not necessary. More important is the ability to visualize the quality of reduction of the posterior capsulotenodesis into the defect, from within the joint, as the sutures are being tied. Clinical and Surgical Pitfalls • After preparation of the anterior capsulolabral tissues, the humeral head is translated anteriorly and perched on the glenoid rim. The Hill-Sachs defect is prepared, and anchors are inserted into its base via an 8-mm cannula placed through the posterolateral accessory portal. Extreme care should be taken to ensure an optimal trajectory of suture anchor insertion. If a poor line is taken, there is a risk of anchor penetration of the anterior humeral head cartilaginous surface. • Neither of the two suture limbs exiting via the posterolateral portal should be used as the posts during arthroscopic knot tying, as the resultant knot will end up within the joint and the quality of remplissage will be reduced. Recurrence rates of up to 15% have been reported after arthroscopic labral repair for anterior shoulder instability.1 Patient age and activity level, soft tissue quality, and the presence of glenoid or humeral bone loss have been identified as predisposing factors.2 A number of potential therapeutic options exist for the management of humeral lesions that are contributing significantly to the instability complex. These include open matched osteoarticular allograft transplantation, transhumeral bone grafting, humeroplasty, rotational humeral osteotomy, and partial or complete humeral head resurfacing.3–7 In arthroscopic Hill-Sachs remplissage (AHSR), a procedure pioneered by Wolf,8 adapted from the open technique described by Connolly,9 the infraspinatus tendon and posterior capsule are used to fill the humeral defect. The term remplissage derives from the French verb remplir, meaning “to fill.” This posterior capsulotenodesis is not intended as an isolated procedure, but rather is always performed in combination with an anterior soft tissue repair. Through “filling” of the defect, the defect is rendered extra-articular and thus is prevented from engagement with the glenoid. In addition, the infraspinatus tendon and capsule act as a checkrein, preventing anterior humeral head translation10 (Fig. 17-1). History and Physical Examination Signs of anterior and inferior apprehension and hyperlaxity are sought. Anterior hyperlaxity is present if the examiner can easily subluxate the humeral head out of the socket in the anteroposterior (AP) direction on drawer testing or if passive external rotation is greater than 85 degrees with the patient’s arm at his or her side. Inferior hyperlaxity is assessed with sulcus sign testing and the hyperabduction test, the result of which is positive with a minimum of 20 degrees of asymmetrical abduction at the glenohumeral joint.11 The presence of skin striae can be a subtle but useful finding suggestive of a predisposition toward soft tissue laxity. To assist in the surgical decision-making process for cases of anteroinferior instability, a preoperative scoring system—the instability severity index score (ISIS)—was developed.12 It enables selection of patients at high risk for treatment failure after isolated arthroscopic Bankart repair. Six risk factors, shown to predict an increased recurrence rate after surgery, were integrated into a 10-point scale (Table 17-1). A score of 3 or fewer points correlates with an acceptable postsurgical recurrence risk of 5% and therefore potential suitability for isolated arthroscopic Bankart repair. For a score of 4 to 6, the recurrence risk is 10%; risk of recurrence rises to 70% with a score over 6. The associated soft tissue and osseous defects dictate the supplemental procedure, performed in addition to a Bankart repair, required to minimize recurrence in patients with an ISIS score higher than 3 (Fig. 17-2). In the senior author’s practice, a combined arthroscopic Bankart and Hill-Sachs remplissage (BHSR) procedure is performed for approximately 10% of cases requiring surgical treatment of anterior shoulder instability.
Arthroscopic Remplissage for Management of Engaging and Deep Hill-Sachs Lesions
Preoperative Considerations
Instability Severity Index Score
Related posts:
 Patient Positioning, Portal Placement, Normal Arthroscopic Anatomy, and Diagnostic Arthroscopy
Patient Positioning, Portal Placement, Normal Arthroscopic Anatomy, and Diagnostic Arthroscopy
 Osteochondral Autograft for Cartilage Lesions of the Knee
Osteochondral Autograft for Cartilage Lesions of the Knee
 Arthroscopic Rotator Cuff Repair: Double-Row Techniques
Arthroscopic Rotator Cuff Repair: Double-Row Techniques
 Surgical Treatment of Posterolateral Instability of the Elbow
Surgical Treatment of Posterolateral Instability of the Elbow
 Primary Repair of Osteochondritis Dissecans in the Knee
Primary Repair of Osteochondritis Dissecans in the Knee
 Arthroscopic Meniscus Repair: All-Inside Technique
Arthroscopic Meniscus Repair: All-Inside Technique
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Arthroscopic Remplissage for Management of Engaging and Deep Hill-Sachs Lesions
 Video
Video