Fig. 22.1
Clinical photo of volar ganglion
Routinely a wrist X-ray evaluation is indicated to rule out preexisting osseous lesions. An Ultrasound imaging study of the wrist is also examined to confirm the diagnosis, as well as to localize the ganglion (Fig. 22.2).
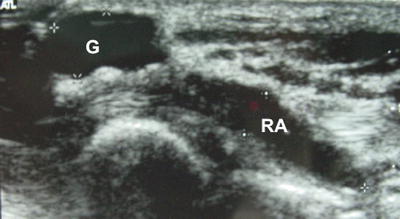
Fig. 22.2
Ultrasound appearance of volar cyst
The MRI of soft tissue masses of the wrist is useful to differentiate them. Ulnar volar ganglions are associated with tears of triangular fibro cartilage complex. An MRI in some circumstance helps to locate the stalk, other lesions, and in the diagnosis of occult ganglia.
Revision of Literature
There is a real deficit of studies of higher methodological quality, and the necessity of more studies to ensure the best prediction of outcomes in wrist arthroscopy [9].
We reviewed the literature on arthroscopic resection of volar wrist ganglion. The publication dates ranged from 2001 to 2012 (Table 22.1). Only one was a prospective randomized study; the authors compared the open resection and arthroscopic resection. All of the other studies were level IV of evidence [10–17].
Table 22.1
Studies reporting recurrence rates and complications of arthroscopic resection of a volar wrist ganglion
Authors | Title | Year | Study design | Evidence | Wrist operated | Average age | Gender | Follow up (months) | Recurrence | Complications | |
|---|---|---|---|---|---|---|---|---|---|---|---|
1 | Ho et al. | Current treatment of ganglion of the wrist | 2001 | Case series | IV | 6 | 38 | 16.4 | 0 (0 %) | 01 no connection with the ganglion was found (16.66 %) | |
2 | Mathoulin et al. | Arthroscopic resection of wrist ganglia | 2004 | Case series | IV | 32 | 46 | 27W | 26 | 0 (0 %) | 01 volar hematoma (3.12 %) |
05M | |||||||||||
3 | Rocchi et al. | Resezione artroscopica delle cisti artrogene dorsali e volari del polso. Nostra esperienza e evalutazioni cliniche | 2005 | Case series | IV | 7 | – | – | 18 | 0 (0 %) | 01 neuropraxia dorsal radial nerve (14.28 %) |
4 | Ho et al. | Arthroscopic volar wrist ganglionectomy | 2006 | Case series | IV | 21 | 48.6 | 11W | 56 | 2 (9.52 %) | 05 no connection with the ganglion was found (23.80 %) |
10M | |||||||||||
5 | Mathoulin and Massarella | Therapeutic interest of wrist arthroscopy about 1,000 cases | 2006 | Case series | IV | 66 | 42 | 53W | 32 | 0 (0 %) | 02 volar hematoma and 01 partial lesion of median nerve (4.54 %) |
13M | |||||||||||
6 | Rocchi et al. | Results and complications in dorsal and volar wrist ganglia arthroscopic resection | 2006 | Case series | IV | 17 | – | – | 15 | 1 (5.88 %) | 01 lesion radial artery (5.88 %) |
7 | Rocchi et al. | Articular ganglia of the volar aspect of the wrist: Arthroscopic resection compared with open excision. A prospective randomized study | 2008 | Prospective randomized study | I | 25 | 37 | 18W | 24 | 3 (12 %) | 01 neuropraxia dorsal radial nerve and 01 lesion radial artery (8.00 %) |
07M | |||||||||||
8 | Rhyou et al. | Arthroscopic resection of volar ganglion of the wrist joint | 2010 | Case series | IV | 9 | 43 | 07W | 15 | 0 (0 %) | 01 partial lesion of median nerve (11.11 %) |
2M | |||||||||||
9 | Chen et al. | Arthroscopic ganglionectomy through an intrafocal cystic portal for wrist ganglia | 2010 | Case series | IV | 3 | 30 | 03W | – | 0 (0 %) | 01 transient paresthesia radial nerve, resolution 1 month (33.33 %) |
00M | |||||||||||
10 | Ostermann | Symposium 4–Excellence in wrist arthroscopy: extending our horizons. Arthroscopic volar ganglionectomy | 2010 | Case series | IV | 26 | 37 | – | – | 4 (15.38) | No |
11 | Langner et al. | Ganglions of the wrist and associated triangular fibrocartilage lesions: A prospective study in arthroscopically treated patients | 2012 | Case series | IV | 20 | 40 | – | 12 | 4 (20 %) | No |
A total of 232 wrists were submitted to an arthroscopic resection. The same operative technique described by Ho et al. [18, 19] was used by all authors. One author included an intrafocal cystic portal [13].
The mean age of patients described in eight articles was 40.45 years. All reported a major incidence in women with a female:male ratio of 3:1. Of nine articles, the follow-up ranged from 12 months to 56 months with a mean of 23.82 months.
There were 14 recurrences. The recurrence rate ranged from 0 % to 20 % with mean of 6.03 %.
There were 16 (6.89 %) related complications. No connection of the complication with the ganglion was described in six wrists [18, 19]. Volar hematoma was described in three patients [20, 21]. Partial lesions of the median nerve were reported in two articles [12, 21], two lesions of a branch of the radial artery [10, 11], and neuropraxis of the superficial radial nerve [10, 13, 19]. Osterman (in the 65th Annual Meeting of the American Society for Surgery of the Hand 2010) and Langner et al. [14] did not report any complications. No patient had loss of arc range of motion.
In a study of five patients of Rocchi et al. [10] the recurrence and complications were higher for midcarpal ganglions.
Recently, Langner et al. reported that patients with volar painful ganglions of the wrist and a positive ulnocarpal stress test are highly associated with TFCC abnormalities [14].
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


