Arthroscopic Management of Fractures Around The Knee
Arthroscopic Management of Fractures Around The Knee
Roberto Rossi
Davide Edoardo Bonasia
Filippo Castoldi
The use of arthroscopic and arthroscopic-assisted techniques for the treatment of fractures around the knee has become more popular over the last decades. Nevertheless, limited types of fractures are amenable to arthroscopy (some tibial plateau fractures, tibial spine avulsions, and osteochondral lesions) and open surgery still remains the gold standard in several cases (i.e., patellar, femoral condyles, and complex tibial plateau fractures). The treatment of osteochondral lesions has been previously described, and this chapter will be mainly focused on arthroscopic treatment of tibial plateau fractures and tibial spine avulsions.
TIBIAL PLATEAU FRACTURES
Clinical Evaluation
Tibial plateau fractures represent only 1% of all fractures (1). They commonly result from varus/valgus stresses across the knee joint, direct traumas, or excessive axial loads to the extended lower limb. They mainly occur in motor vehicle accidents (i.e., bumper trauma and motorcycle accidents), in sports (i.e., skiing and high-contact sports) and falls from height.
A correct classification of the fracture is mandatory for the decision-making and to assess the prognosis. We commonly use Schatzker’s classification. Its advantages compared with other classification systems (i.e., Hohl, Moore, Honkonen and Jarvinen, AO, etc.) include handiness as well as a good correlation with severity, treatment, and prognosis of the fracture (2). Type I is a wedge fracture of the lateral hemiplateau, without articular depression. Type II is a wedge fracture of the lateral hemiplateau associated with articular depression. Type III is an isolated articular depression fracture involving the lateral plateau. Type IV is a medial tibial plateau fracture, most likely associated with tibial eminence fracture. Type V is a bicondylar tibial fracture, without metaphyseal involvement. Type VI is an unicondilar or bicondilar tibial fracture, with metaphyseal involvement.
Clinically, the traumatic mechanism should be investigated, a dislocation excluded and the physical examination should be mainly focused on the neurovascular evaluation and assessment of possible associated lesions. The knee is usually swollen as well as painful and stability maneuvers must be carried out under anesthesia, before surgery.
For a correct assessment of the fracture type, the workup must include anteroposterior (AP) and lateral X-ray views as well as a CT scan of the involved knee. MRI is not routinely required, but may be useful when associated ligamentous injuries are suspected, even though ligaments reconstruction is usually delayed untill after fracture healing.
Treatment
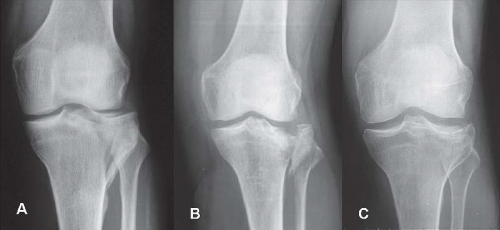
The management of the fracture depends on several factors and these include (1) fracture configuration (2); concomitant soft-tissue injury (3); patient’s age and activity level; and (4) bone quality. Arthroscopic reduction and internal fixation (ARIF) is indicated in Schatzker type I to III (Fig. 84.1), when the displacement is more than 5 mm, in compliant patients and in nonarthritic knees (Table 84.1). Nevertheless, in some Schatzker type II fractures, if the bone quality is poor or the wedge fragment is comminuted, open reduction and internal fixation (ORIF) with plating is recommended.
Arthroscopic-assisted techniques have been described for Schatzker type IV fractures (wedge medial plateau fragment, with an additional fragment involving the tibial eminences). These fractures usually result from high-energy traumas, with soft-tissue injuries (skin, ligaments, and capsule) and are more difficult to reduce by external maneuvers. Therefore, we recommend ORIF in these cases to avoid as well possible arthroscopic fluid leakage in the soft tissues.
Many open and arthroscopic-assisted techniques have been proposed. All of them allow a direct visualization of fracture reduction and a precise evaluation and treatment of associated intraarticular lesions, with a minimally invasive procedure. They generally have in common the indirect reduction through an en masse elevation of the depressed fragment (Schatzker type II to IV) from below the involved hemiplateau, using a bone punch. Nevertheless, they differ in the type of fixation and in the way of filling the metaphyseal void under the fracture. Recent studies advocate the use of PMMA (polymethylmethacrylate) or bone substitutes such as carbonate apatite or calciumphosphate cement, instead of autologous iliac crest graft, to reduce donor site morbidity and permit early weight-bearing. Nevertheless, with bone substitutes, the disadvantages are high cost as well as less osteoinductive and osteoconductive properties, and with acrylic cement, the risk of thermal osteonecrosis should be considered.
FIGURE 84.1. Tibial plateau fractures amenable to ARIF include Schatzker A: type I, B: type II, and C: type III fractures.
Table 84.1 Indications for proximal tibial fractures
Fracture Type (Schatzker Classification)
Treatment
Type I (lateral plateau wedge fracture, without articular depression)
ARIF and percutaneous lag screw fixation
Type II (lateral plateau wedge fracture with articular depression)
ARIF and percutaneous lag screw fixation vs ORIF and plating (if poor bone quality or high comminution of the wedge fragment)
Type III (lateral plateau articular depression only)
ARIF and percutaneous lag screw fixation
Type IV (medial tibial plateau fracture with tibial eminence fracture)
ORIF and plating vs ARIF and percutaneous lag screw fixation (if low energy trauma and isolated involvement of the medial plateau, either wedge or depressed fragment)
Type V (bicondylar tibial fracture, without metaphyseal involvement)
ORIF and double plating vs external fixation
Type VI (unicondilar or bicondilar tibial fracture, with metaphyseal involvement)
ORIF and double plating vs external fixation
Authors’ Preferred Technique
To overcome the necessity of using bone graft or substitutes, we proposed an alternative arthroscopic-assisted technique (1, 3) for Schatzker types II and III fractures.
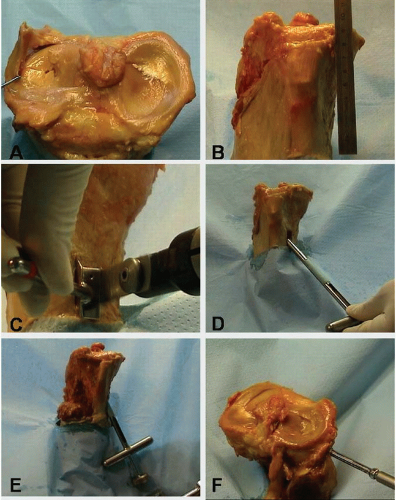
The patient is positioned supine in general or spinal anesthesia, with the tourniquet placed on the proximal thigh. The knee stability is then evaluated under anesthesia. Arthroscopic examination is performed using gravity inflow, through classical anteromedial and anterolateral portals. The heamarthrosis is drained and any osteochondral fragments removed. The degree of fracture depression and soft-tissues injury is assessed. A longitudinal 3-cm skin incision is made on the medial aspect of the tibia, starting 10 cm from the articular surface and extended distally. A cortical window (10 × 20 mm) is opened on the medial tibia and a hollow trephine cutter (diameter 10 mm), with a sawtoothed tip, is introduced in the tibia itself (Figs. 84.2 to 84.4).
FIGURE 84.2. In this human specimen, ARIF for lateral tibial plateau fractures is shown (A). On the anteromedial tibia, 10 cm below the articular surface (B), a cortical window is opened (C). A cannulated cutter is inserted in the cortical window (D) and positioned 2 cm below the lateral plateau. A bone tamp is inserted in the cutter and the fracture reduced (E). Two or three cannulated screws are inserted percutaneously from lateral to medial (F).
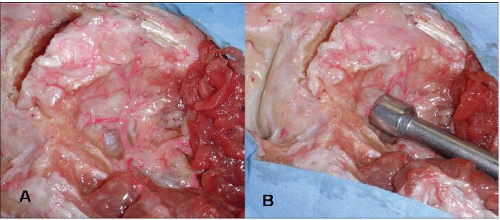
FIGURE 84.3. This human specimen shows the vascularity of the lateral tibial plateau (A) that can be damaged by inserting the bone tamp (B) in the lateral column and not in the medial one.
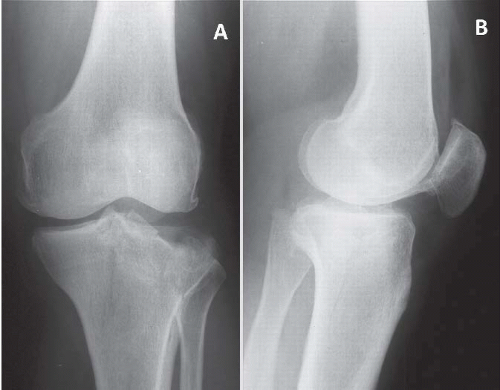
FIGURE 84.4. Schatzker type II fracture in AP (A) and lateral view (B).
Under fluoroscopic control (AP and lateral views), the edge of the cutter is placed 2 cm below the lateral plateau fracture (Fig. 84.5). A bone punch (diameter 9 mm) is then inserted into the cutter and, with a hammer, the cancellous bone block (base 9 mm diameter, height about 100 mm) is impacted under the fracture to obtain an indirect reduction (Fig. 84.2). If the articular surface is severely compacted, this procedure could be repeated placing the cutter in another direction, through the same window. The anatomical reconstruction of the articular surface is assessed arthroscopically (Fig. 84.6). Once the optimal reduction is achieved, the fracture is then fixed with two or three cancellous cannulated screws (6.5 mm), inserted percutaneously from lateral to medial and 1 cm under the articular surface (Fig. 84.2). The cutter and the punch are then removed and the tibial cortex replaced in situ (1). Neither iliac crest graft nor bone substitutes are used with this technique.
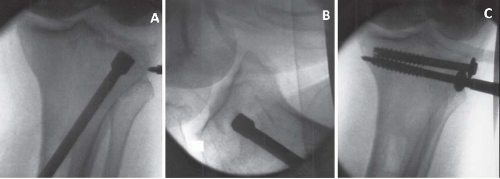
FIGURE 84.5. Same case of Figure 84.4. A: Fluoroscopy in AP (A) and lateral (B) view of fracture reduction using the bone tamp from medial to lateral. C: Fluoroscopy of synthesis with cannulated screws.
In Schatzker type I fractures (wedge fractures, without articular surface depression), the en masse elevation is not required and, under arthroscopic control, the wedge fragment is usually reduced by external maneuvers. These include a digital compression on the wedge fragment that is usually distally displaced, a varus stress on the knee (playing on the ligamentotaxis by the articular capsule) and the use of a K wire as a joystick. Once the fracture is reduced and the articular surface restored, a percutaneous fixation with screws is performed, as previously described.
Complications, Controversies, and Special Considerations
The advantages of this technique include (1) preserving the fractured lateral tibial column from further surgical damages (i.e., cortical window opening and cancellous bone mobilization) (2); preserving the lateral plateau blood supply (Fig. 84.3) (3); playing on the inclined plane effect of the tunnel (that is oblique from medial to lateral and not vertical right below the depressed plateau); and, therefore (4), avoiding bone or bone substitutes augmentation.
Only gold members can continue reading. Log In or Register to continue
 Acromioclavicular Separations: Arthroscopic Reconstruction of The Acromioclavicular Joint
Acromioclavicular Separations: Arthroscopic Reconstruction of The Acromioclavicular Joint



