Arthroscopic and Open Primary Repair of Acute Thumb Metacarpophalangeal Joint Radial and Ulnar Collateral Ligament Disruptions
Alejandro Badia
Prakash Khanchandani
DEFINITION
Ulnar collateral ligament (UCL) and radial collateral ligament (RCL) tears of the thumb metacarpophalangeal joint (MCP) are common injuries resulting from disruption of the continuity of these ligaments.
These disruptions are frequently the result of an athletic injury, a fall, or a motor vehicle accident.
ANATOMY
The MCP joint of the thumb is transitional between a condyloid and ginglymus joint. The articulating surface of the base of the proximal phalanx is a shallow concavity that provides relatively little intrinsic stability. Hence, most of the joint’s stability is afforded by its ligament and capsular supports.
The RCL and UCL are both structurally similar, composed of both proper and accessory components, and are the main stabilizers of the thumb MCP joint.27
The proper collateral ligaments, which originate from a fossa in the metacarpal neck dorsal to the axis of rotation, are the primary ligamentous supports. They fan out from their proximal origins to distal insertions on the lateral and volar aspects of the base of proximal phalanx.
The accessory collateral ligaments act as supplementary supports originating from the palmar aspect of the metacarpal neck fossa and inserting into the volar plate and the sesamoid on respective sides of the joint.27
The collateral ligaments provide not only medial and lateral stability but also stability in the dorsovolar plane by virtue of their dorsal origin and their volar insertion.26
The volar plate is a central fibrocartilaginous structure extending from the neck of the metacarpal proximally to the base of the proximal phalanx distally.
One difference between the ulnar and radial sides of the MCP joint is related to the aponeurosis. The broad abductor aponeurosis covers the entire radial side of the MCP joint, whereas the much narrower adductor aponeurotic sheath spans the ulnar side of the joint.
PATHOGENESIS
Acute injury of the UCL usually results from sudden forceful abduction and extension at the thumb MCP joint.21,25
This can take place during a fall on an outstretched hand with the thumb abducted, as seen in skiers,8 or in baseball players when the glove strikes the ground while fielding.
The extent of the injury and the grade of the injury depend on the loading force at the time of impact. The most common injury of the thumb MCP joint is a partial disruption or sprain of the UCL.
Tears of the UCL can occur anywhere within the ligament’s substance, although most take place at or near the site of insertion into the proximal phalanx, sometimes with an avulsion fracture (FIG 1A).4,9,28
RCL injuries are generally caused by sudden adduction and extension of the MCP joint, commonly occurring during athletic injuries.5 They can also occur by direct blunt impact to the lateral side of the thumb.
The RCL is more often injured close to its origin on the dorsoradial metacarpal head. It may also be disrupted in its midsubstance.
NATURAL HISTORY
Untreated UCL injuries are relatively common. Patients are often sent away being told they simply have a “sprain.” If instability is present and not corrected, the patient may experience pinch weakness and eventually chronic pain.
Untreated RCL tears are even more common and often result in late degenerative arthritis, commonly requiring MCP arthrodesis.
Less severe avulsions may lead to prominent osteophytes on the dorsoradial aspect of the metacarpal neck, suggesting the prior injury.
Mondry19 first described the unstable thumb MCP joint in 1940, whereas Watson-Jones30 mentioned the importance of the UCL in relation to stability of the MCP joint of the thumb.
Campbell6 described gamekeeper’s thumb as a chronic instability of the UCL in Scottish gamekeepers.
Gerber et al13 popularized the term skier’s thumb to refer to acute UCL injuries.
Stener28 outlined the ligamentous anatomy of the thumb MCP joint and subsequent pathoanatomy of the lesion now termed the Stener lesion. Stener also described
avulsion of the UCL leading to articular fracture of the proximal phalanx, now popularly referred to as a bony gamekeeper’s thumb.29
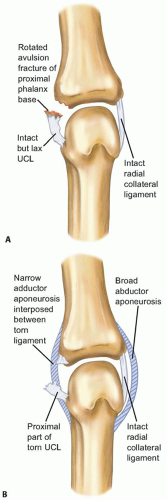
FIG 1 • A. A bony gamekeeper’s thumb. B. The narrow adductor aponeurosis is interposed between the avulsed ligament-bone and the site of attachment.
Frank and Dobyns12 reported that RCL injuries are somewhat more common than initially thought, with incidences ranging from 23% to 35% of collateral ligament injuries.
This has echoed our experiences with the more subtle RCL injuries often being neglected, causing late morbidity.
PATIENT HISTORY AND PHYSICAL FINDINGS
Ulnar Collateral Ligament Tears
Patients with UCL tears present with pain, stiffness, tenderness, and swelling of the MCP joint. The defining symptom, however, may be marked pinch weakness.
On examination, there is discrete tenderness over the ulnar joint line, at the ulnar side of the metacarpal neck, and most classically at the volar ulnar base of the proximal phalanx.2
Physical examination is critical in establishing the need for surgical treatment by distinguishing between a partial and a complete ligament tear.
A valgus stress examination comparing the stability of the injured versus the uninjured UCL is the best method to detect a complete tear.
The stress test may be aided by live fluoroscopy and the use of a local anesthetic block.
The presence of an associated fracture should not deter the examiner from performing a stress test. Nondisplaced avulsion fractures at the insertion site of the proper collateral ligament may coexist with a complete ligament tear.
The results of the stress test are based on angular instability of the joint and the quality of the “end point.”
Laxity of more than 30 degrees in extension and 15 degrees in flexion as compared to the contralateral side should be highly suggestive of a complete tear of the UCL.15
The presence of fullness or a palpable mass on the ulnar aspect of the metacarpal head and neck, representing a Stener lesion,1 is strongly suggestive of a completely disrupted and retracted UCL.
Volar subluxation of the MCP joint signifies loss of the dorsal volar stabilizing effect of the collateral ligament and is also consistent with a complete tear.
Radial Collateral Ligament Tears
RCL tears present as localized tenderness over the radial base of the proximal phalanx but more commonly over the metacarpal head.
The dorsoradial aspect of the metacarpal head may be prominent due to soft tissue swelling.
Acute RCL injuries are assessed in the same manner as discussed for UCL injuries.
For the stress test of the RCL in extension and 30 degrees of flexion, laxity of the joint greater than 30 degrees as compared to the uninjured side suggests a complete tear of the RCL.Related posts:
 Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
Volar Plating of Distal Radius Fractures
Ligament Stabilization of the Unstable Thumb Carpometacarpal Joint
Operative Treatment of Metacarpal Fractures
Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
Volar Plating of Distal Radius Fractures
Ligament Stabilization of the Unstable Thumb Carpometacarpal Joint
Operative Treatment of Metacarpal Fractures

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


