Radiocarpal Fracture-Dislocations
Chris J. Williamson
Asif M. Ilyas
DEFINITION
The radiocarpal joint’s stability is provided by the carpal articulation at the scaphoid and lunate fossae as well as the soft tissue restraints of the capsule and extrinsic radiocarpal ligaments.
Radiocarpal dislocations occur through a traumatic separation of the proximal carpal row from the articular surface of the distal radius.
Radiocarpal dislocations can occur in either a volar or dorsal direction, with the most common direction being dorsal.
Radiocarpal dislocations can occur with only soft tissue disruption or, more commonly, in association with marginal rim fractures of the distal radius or ulnar styloid.
Radiocarpal dislocations are often confused with distal radius fractures of the marginal rim or volar/dorsal shear fractures (ie, “Barton” fractures) (FIG 1).
Radiocarpal dislocations represent a shear or avulsion injury of the wrist that may or may not be associated with an avulsion fracture of the distal radius or ulna (FIG 1A).
Barton fractures of the distal radius represent compression and/or shear fractures (FIG 1B).
Two classification systems are typically used to describe radiocarpal dislocations.
Moneim et al13 classified radiocarpal dislocations based on the presence or absence of an intercarpal ligament injury.
Type 1 dislocations do not have an associated intercarpal injury.
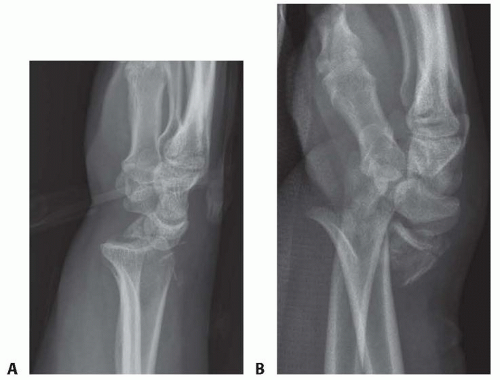
FIG 1 • Radiocarpal dislocations can be confused with shear fractures of the distal radius. A. Note the disruption of the carpus from the distal radius in this lateral view of a radiocarpal fracture-dislocation. In contrast, (B) note in this lateral view of this distal radius fracture that the relationship between the carpus and distal radial articular surface is maintained.
Type 2 injuries are associated with a concomitant scapholunate ligament.13
Dumontier et al4 classified radiocarpal dislocations based on the presence or absence of an associated avulsion fracture off the radial styloid.
Type 1 injuries are considered purely ligamentous with minimal cortical avulsion off the radial styloid.
Type 2 injuries are associated with a large radial styloid fracture compromising of at least one-third of the scaphoid fossa.4
ANATOMY
The average arc of motion in a normal wrist ranges from 68 degrees of flexion to 50 degrees of extension.10
Radiocarpal joint stability is provided by both the osseous joint articulation between the scaphoid and lunate bones and their corresponding fossae of the distal radius, along with the extrinsic radiocarpal ligaments and the wrist capsule (FIG 2).
Among the various volar radiocarpal ligaments, the primary ligaments important to radiocarpal stability are the short radiolunate and the radioscaphocapitate ligaments.
The short radiolunate ligament originates from the stout margin of the lunate facet of the volar distal radius and serves as the primary restraint against volar translation of the carpus.
The stout radioscaphocapitate ligament originates from the radial styloid and resists ulnar translation of the carpus.
The ulnocarpal ligaments, including the ulnolunate and the ulnotriquetral ligaments, take their origin from the ulnar styloid. Along with the triangular fibrocartilage complex (TFCC), they assist in providing radiocarpal and ulnocarpal joint stability.
The dorsal radiocarpal ligaments are highly variable12 and also assist in imparting stability to the radiocarpal joint, although to a much lesser extent than the volar radiocarpal ligaments.
PATHOGENESIS
Radiocarpal dislocations can occur in either a volar or dorsal direction, with dorsal being far more common (˜85%).4
The injury requires pronation and hyperextension of the wrist with a shear force across the joint. With increasing amounts of supination, the risk of a perilunate dislocation rather than a radiocarpal dislocation increases.11
Disruption of the radiocarpal ligaments, the most critical of which are the radioscaphocapitate and the short radiolunate, is necessary to dislocate the radiocarpal joint.
A pure dislocation without a bony injury is less common. More often, a fracture of the radial styloid, volar marginal rim, or ulnar styloid is identified representing an avulsion of the origin of the radioscaphocapitate, short radiolunate, or ulnocarpal ligaments, respectively.
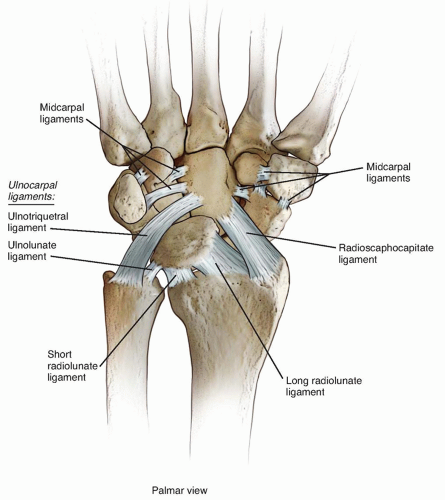 FIG 2 • The extrinsic volar radiocarpal ligaments of the wrist include radioscaphocapitate (RSC), long radiolunate (LRL), short radiolunate (SRL), ulnolunate (UL), ulnotriquetral (UT) ligaments. |
NATURAL HISTORY
Mechanisms of injury are typically falls from a height, industrial injuries, and motor vehicle accidents.
The incidence of radiocarpal dislocations has been published to be as low as 0.2%5 of all hand and wrist dislocations.5 More recent studies have found incidence of radiocarpal dislocations to be as high as 2.7% of all distal radius fractures and wrist dislocations.9
Due to the high-energy nature of these injuries, there is a high association of associated injuries including neurologic injuries, vascular injuries, and open wounds.1,4,13
Residual radiocarpal instability and posttraumatic wrist degeneration is common, particularly with purely ligamentous injuries (Dumontier type 1).4
PATIENT HISTORY AND PHYSICAL FINDINGS
Radiocarpal dislocations typically present with a very swollen and painful wrist, with likely deformity (FIG 3).
Physical examination should include a thorough neurologic, vascular, and tendon examination.
Neurologic deficits, particularly of the median nerve, are common with displaced radiocarpal dislocations.

FIG 3 • Typical deformity following a dorsally displaced radiocarpal dislocation.
Vascular embarrassment to the hand may occur with prolonged displacement and swelling.
Incarceration of the dorsal extensor tendons can occur pre- and postreduction.
Close inspection of the skin should also be performed, as open wounds can also be present possibly signifying an open arthrotomy of the wrist or an associated open fracture.16
IMAGING AND OTHER DIAGNOSTIC STUDIES
Evaluation should begin with plain radiographs including a posteroanterior and lateral views of the wrist (FIG 4). Additional oblique views can help in assessment.
On the lateral view, the radiograph should be scrutinized for the alignment of the arcs of Gilula, representing the relationship between the midcarpal and radiocarpal joints. Disruption between the lunate and the distal radius signifies a radiocarpal disruption, whereas disruption between the capitate and lunate may represent a perilunate injury (FIG 5).
On the posteroanterior view, the radiograph should be scrutinized for associated avulsion fractures of the distal radius or ulna, ulnar translation of the carpus relative to the distal radius, and intercarpal diastasis.
Computed tomography (CT) may be helpful in identifying marginal rim fractures and to further evaluate intra-articular fracture patterns (FIG 6).Related posts:
 Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
Volar Plating of Distal Radius Fractures
Ligament Stabilization of the Unstable Thumb Carpometacarpal Joint
Dorsal Block Pinning of Proximal Interphalangeal Joint Fracture-Dislocations
Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
Volar Plating of Distal Radius Fractures
Ligament Stabilization of the Unstable Thumb Carpometacarpal Joint
Dorsal Block Pinning of Proximal Interphalangeal Joint Fracture-Dislocations

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


