Arthrodesis of the First Metatarsophalangeal Joint
Arthrodesis of the First Metatarsophalangeal Joint
Gerard V. Yu
Jeffrey E. Shook
Procedures designed to treat disorders involving the first metatarsophalangeal joint may be categorized as soft tissue or muscle-tendon balance, exostectomy or cheilectomy, osteotomy, resection arthroplasty, implant arthroplasty, or arthrodesis. Within the orthopedic community, first metatarsophalangeal fusion is a time-honored procedure for the treatment of hallux rigidus and geriatric hallux valgus. Until recently, this procedure was not favored among podiatric physicians. This was largely because of interest in resection and implant arthroplasty and a lack of familiarity with arthrodesis. The concept of eliminating motion at the first metatarsophalangeal joint has been viewed as unacceptable because hallux limitus or rigidus creates distinct mechanisms of compensation that may lead to other symptoms in some patients. In addition, investigators believed that normal function and motion at the first metatarsophalangeal joint were necessary to provide a stable medial column for propulsion and a normal heel-to-toe gait cycle. However, greater appreciation for the complications associated with resection or implant arthroplasty has fueled interest in first metatarsophalangeal joint arthrodesis.
Until 1990, only two publications concerning first metatarsophalangeal arthrodesis can be identified in the podiatric literature (1,2). Since 1990, multiple publications have been released from the podiatric community (3, 4, 5, 6, 7, 8, 9, 10, 11, 12). Increased interest and improved technique have expanded the accepted indications for this procedure because of predictable results. Arthrodesis is an effective and powerful procedure for addressing a multitude of disorders affecting the first metatarsophalangeal joint. When performed correctly in the appropriate patient population, this procedure stabilizes the forefoot and increases the function of the medial column, and it often produces a pain-free gait.
Fusion of the first metatarsophalangeal joint was first described by Broca in 1852 (13). Subsequently, in 1894, Clutton reported on seven procedures performed on four patients. The procedure rendered excellent results even in a postal worker. Clutton surmised that “anchylosis” of the joint in the “ideal position” would produce the most permanent and satisfactory correction for a hallux valgus deformity (14). Although little was published concerning this procedure for the next 50 years, Clutton’s sentiments have been reiterated by a resurgence in the popularity of arthrodesis of the first metatarsophalangeal joint evinced by multiple studies of this procedure from 1940 to the present (1-60).
Early interest in this procedure evolved from serendipitous findings after ankylosis at the first metatarsophalangeal joint was produced after an infectious process (40,48). In 1941, McKeever encountered a successful fusion of the first metatarsophalangeal joint after a complication of a bilateral bunionectomy. Infection produced a functional arthrodesis on one foot. This side had a better result, both subjectively and objectively, than the nonfused, contralateral bunionectomy. Specifically, metatarsus primus varus was noted to be greater after the standard bunionectomy. Subsequently, McKeever performed this procedure on military personnel and was so impressed with the results that he adopted this procedure for all cases of hallux valgus, hallux rigidus, and metatarsus primus varus (40).
Since McKeever’s original article, 29 separate studies involving 10 or more surgical procedures have been published in the English language literature (Table 1). The position of fusion is the most critical aspect of the operation. Unfortunately, for some authors, the focus of the procedure has been oriented toward resection techniques and fixation modalities implemented to ensure arthrodesis, rather than the position of fusion.
Along with advances in technique has been expansion in the indications commonly used for fusion of the great toe joint. Traditionally, this procedure was performed for cases of hallux rigidus and geriatric hallux valgus. Currently, arthrodesis of the first metatarsophalangeal joint is used in cases of inflammatory or septic arthritis, traumatic arthritis, hallux varus or recurrent hallux valgus, failed resection or implant arthroplasty, and neuromuscular instability or spasticity. Despite the technical advances and greater use of the procedure, fusion rates have not been significantly altered over the years. Regardless of the specific approach to joint preparation or the type and method of fixation, the result of the fusion most closely mirrors the success or failure in positioning of the hallux. This is best illustrated by the uniformity of good results with appropriate position in almost every type of technique described for the performance of arthrodesis of the first metatarsophalangeal joint since over the past century.
A good sense of the patient’s expectations is important in an evaluation for first metatarsophalangeal joint arthrodesis. This is especially true with regard to activity level, occupation, and desired shoe gear. Patients who run or play racquet sports such as tennis and racquetball may function well after first metatarsophalangeal arthrodesis, whereas a bowler may have great difficulty. A person whose occupation requires a greater than normal need for squatting, such as a plumber, may be at a great disadvantage with first metatarsophalangeal joint arthrodesis or may require a greater than average amount of dorsiflexion at the time of fusion. Thus, patients need to understand the implications of first metatarsophalangeal joint fusion with respect to activities of daily living, participation in sports or other strenuous types of occupations or activities, and limitations with shoe gear. In cases of revisional surgery, awareness of patient goals with respect to pain relief, cosmesis, and function may direct the physician toward arthrodesis and away from extraarticular reconstruction.
An apropulsive or antalgic gait, in which minimal or no motion is seen through the first metatarsophalangeal joint, may be a good indicator that the patient is likely to do well with an arthrodesis. Other concomitant pedal deformities such as contracted digits, hallux extensus or malleus, metatarsus adductus, and collapsing pes valgo planus may be important in the overall management of the foot. Another particular concern is appreciation for the sagittal and transverse plane position of the first metatarsal. An apparent metatarsus primus varus or elevatus may be a result of retrograde forces at the first metatarsophalangeal joint. Restoring the hallux to a more anatomic position may reduce these secondary deformities and may preclude the need for a proximal osteotomy or proximal arthrodesis. When a previous osteotomy has been preformed on the first metatarsal, the need for additional proximal procedures should be studied further and may become necessary to reestablish the weight-bearing capacity of the medial column. Evaluation for proximal pathologic features helps to ensure a good functional result after fusion. Specific problems, such as an equinus deformity or limb length discrepancy, may affect the position of arthrodesis or an ancillary procedure selection.
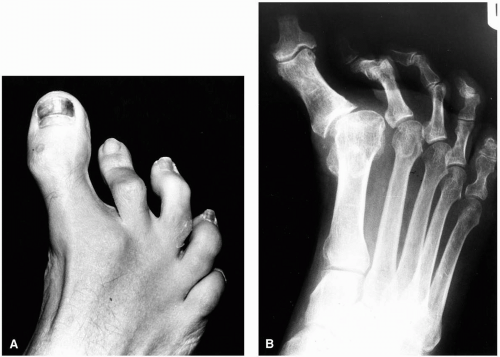
FIG. 1. A,B: Acquired hallux varus deformity in an adult patient with no underlying neuromuscular disease or prior surgical procedures. This condition is difficult to repair, and correction is difficult to maintain using joint salvage techniques.
INDICATIONS
The primary indications for arthrodesis for the first metatarsophalangeal joint have not changed dramatically in the last 50 years; however, the frequency of use of fusion for these conditions has increased significantly. Arthrodesis of the first metatarsophalangeal joint should be considered in two specific instances, regardless of any other contributing factors: significant degenerative changes at the first metatarsophalangeal joint and clinical and radiographic evidence of instability at the first metatarsophalangeal joint (Fig. 1). Often, osteoarticular damage and periarticular instability are seen concomitantly and should not be considered mutually exclusive. Although the overall indications are vast, a common finding with each specific entity may be intraarticular damage of the first metatarsophalangeal joint (including sesamoidal apparatus) or joint instability. Current indications for arthrodesis of the first metatarsophalangeal joint are provided in Table 2; however, this list is not meant to be totally inclusive and does not imply that other surgical procedures are not appropriate for some of the same conditions (12,61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73).
The most common indications for first metatarsophalangeal joint arthrodesis have been geriatric hallux valgus deformity and hallux limitus or hallux rigidus deformities. These two entities account for an overwhelming majority of the clinical indications found throughout the literature (9). Advances in the understanding of the origin of these two deformities, coupled with improved surgical techniques, have limited the use of fusion as the primary treatment of either hallux valgus or hallux limitus or rigidus among many surgeons. Numerous other procedures may be considered first. However, in specific instances, arthrodesis may present a more favorable and predictable outcome compared with reconstructive-type procedures.
Gross instability of the first metatarsophalangeal joint may be a primary indication for fusion regardless of the quality of the joint. We believe that fusion should be considered a primary procedure for correcting an initial hallux valgus deformity in patients with an underlying neuromuscular disease (71,74), severe ligamentous laxity or hypermobility, or severe residual metatarsus adductus (not to be corrected). In these instances, the chance for failure is greater with restoration of musculotendinous balancing around the first metatarsophalangeal joint. Fusion corrects positional deformity and improves function. This is especially true in patients with spastic neuromuscular conditions such as cerebral palsy (Fig. 2).
Renshaw et al. reviewed 14 procedures in 11 patients with cerebral palsy and severe bunion deformities. Soft tissue releases and extraarticular osteotomies demonstrated a propensity for recurrence at long-term follow-up. Arthrodesis of the first metatarsophalangeal joint was recommended as the procedure of choice in this patient population to prevent recurrence (75). The clinician should identify and address any periarticular spasticity or contracture, to decrease the incidence of malunion or nonunion (70). One of the most common causes of nonunion in our experience is underlying neurologic disease and associated spasticity.
TABLE 2.Current indications for arthrodesis of the first metatarsophalangeal joint
Previously failed bunion procedures
Failed implant arthroplasty (hemiarthroplasty or total arthroplasty)
Neuromuscular disease
Cerebral palsy
Previous poliomyelitis
Cerebrovascular accident
Chronic gouty arthritis
Inflammatory arthritis
Rheumatoid arthritis
Psoriatic arthritis
Charcot’s neuroarthropathy
Infection/septic arthritis
Ligamentous laxity
Congenital
Down’s syndrome
Ehlers-Danlos syndrome
Marfan’s syndrome
Hallux abducto valgus deformity
Severe hallux valgus deformity
Moderate hallux valgus deformity with sub-second metatarsal lesion/metatarsalgia
Hallux abducto valgus with concomitant metatarsus adductus
Failed Keller procedure or other resection arthroplasty
Loss of extensor or flexor function
Hallux varus
Congenital
Iatrogenic
Trauma
Joint proper (first metatarsal head and phalangeal base)
Sesamoidal apparatus
Hallux limitus/hallux rigidus
Fusion obviates the need for additional structural correction often required to produce a good, long-standing result in cases of severe hallux abducto valgus deformity. Because of the severity of the bunion deformity associated in patients with disorders such as Down’s syndrome and spastic cerebral palsy, arthrodesis of the first metatarsophalangeal joint represents an excellent choice (71). Although some surgeons prefer arthrodesis of the first metatarsocuneiform joint, we favor fusion at the metatarsophalangeal joint level. These patients may have difficulty in remaining non-weight bearing for 6 weeks after a closing base wedge osteotomy. Early ambulation on an arthrodesis of the first metatarsophalangeal joint is much better tolerated. Alteration of fixation methods (plate application) also enhances the fusion rate with the proper position when early weight bearing is anticipated. This same flexibility does not exist with any basilar osteotomy or proximal fusion needed to correct the significant deformity seen in this patient population.
Patients with ligamentous laxity present a difficult challenge when one attempts to repair a hallux abducto valgus deformity. It is not uncommon to see a postoperative hallux varus after a reconstructive surgical procedure. In fact, many of these patients experience several deviations in hallux position throughout a traditional treatment course. Successful arthrodesis allows for permanent correction and provides enhanced stability to the medial column and perhaps to the rearfoot complex.
Congenital hallux varus, hallux flexus, and hallux malleus deformities, as well as the flail toe, are also indications for fusion of the first metatarsophalangeal joint. Such conditions are commonly reported in patients with underlying neuromuscular disease of paralytic origin, such as poliomyelitis, or after previous surgical procedures of the first ray. An inability to control the hallux with conventional tendon balancing procedures is a primary indication for arthrodesis in most of these situations.
We have found fusion to be a satisfactory procedure for the correction of hallux abducto valgus in patients with moderate to severe residual metatarsus adductus. This is particularly true in older patients, especially if their gait is relatively apropulsive and their activity level is low. In such cases, our experience has been that the conventional hallux valgus procedure often produces less than optimal long-term results. In skeletally mature patients with residual metatarsus adductus, it is often difficult to justify cutting the lateral four metatarsals to provide space for repositioning the first ray, especially when symptoms and clinical findings are isolated to the first ray complex. Arthrodesis of the first metatarsophalangeal joint obtains a permanent position of the hallux. Although the true first intermetatarsal angle does not reduce as much as desired, patient satisfaction is usually obtained. Fusion of the first metatarsophalangeal joint has also greatly improved the alignment of the lesser toes, regardless of whether surgical procedures were performed at the level of the lesser metatarsophalangeal joint and the digits.
Specific attention must be given to the position of fusion in patients with residual metatarsus adductus. One should understand and appreciate the amount of lateral deviation of the lesser digits. Placement of the great toe in what would normally be considered an optimal position may result in a foot with a large space between the hallux and the lesser toes. This can occur in spite of performing soft tissue releases on the lateral aspect of the lesser metatarsophalangeal joints with or without concomitant medial joint plication. Ultimately, the surgeon must determine where the lesser digits will rest after all forefoot procedures have performed.
In dealing with the fully mature adult foot, reconstructive surgery for metatarsus adductus is usually not recommended. Conversely, when dealing with children and residual metatarsus adductus in which there is usually little lesser digit abduction, we have found more conventional procedures, with or without correction of the underlying metatarsus adductus, to be beneficial. In more severe cases, metatarsus adductus is corrected by way of osteotomies of the first through third metatarsals or, more commonly, osteotomies of all five metatarsals. We do not in any way wish to convey that fusion is an appropriate procedure in the child or juvenile patient with metatarsus adductus.
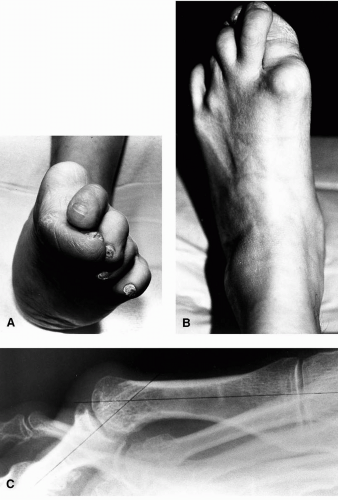
FIG. 2. A-C: Severe spastic hallux abducto valgus deformity secondary to underlying severe cerebral palsy. This is another primary indication for arthrodesis of the first metatarsophalangeal joint.
The treatment of iatrogenic and postoperative complications of first ray procedures is another strong indication for first metatarsophalangeal arthrodesis (76). When surgically treating iatrogenic hallux varus or recurrent hallux abducto valgus deformity, periarticular soft tissue balance cannot be predictably restored in many instances. Moreover, degenerative changes may affect the joint or the sesamoid apparatus. When joint instability and intraarticular damage coexist, a joint-destructive type of procedure is preferred. Revisional surgery requires a slightly different approach than with primary hallux abducto valgus surgery. Some emphasis must be placed on selecting a definitive procedure even if this involves joint destruction in a younger patient. Experience proves to be the most important factor in the decision-making process; however, too many times we have seen multiple attempts at joint preservation when this was not realistic. In many of these instances, fusion was not considered because of a lack of familiarity with the procedure, because of an inability to perform the procedure, or simply because the patient was “too young.” With each subsequent attempt atjoint preservation surgery, many patients invariably end up with an increasing amount of stiffness to the first metatarsophalangeal joint, which may prove extremely painful and nonfunctional. Consequently, even if an appropriate clinical appearance is achieved, the failure to restore motion to the great toe joint results in increased functional disability. Resection or implant arthroplasty may be considered in revisional surgery or iatrogenic deformities, but these procedures do not give the same functional result as fusion and often necessitate another revisional operation. Arthrodesis of the first metatarsophalangeal joint consistently corrects multiplanar deformities and proves to be a reliable procedure to reestablish function of the first ray complex.
Common clinical problems with elements of intraarticular damage are controversial with respect to arthrodesis of the first metatarsophalangeal joint. Specifically, hallux limitus and hallux rigidus are entities with a wide disparity in treatment philosophy among surgeons. Many physicians believe that preservation or re-creation of motion by extraarticular osteotomy or implant arthroplasty is essential in treating hallux limitus and hallux rigidus, respectively. Resection arthroplasty may also be successfully employed in these types of cases. However, arthrodesis should also merit significant consideration in this patient population, especially because this procedure has repeatedly provided consistent, long-term results in these patients. Resection arthroplasty is a viable option and may be more desirable in patients who cannot tolerate the postoperative course after a fusion or who do not want a fusion.
Only gold members can continue reading. Log In or Register to continue
 Anatomic Dissection of the First Metatarsophalangeal Joint for Hallux Valgus Surgery
Anatomic Dissection of the First Metatarsophalangeal Joint for Hallux Valgus Surgery
 Juvenile Hallux Abducto Valgus Deformity
Juvenile Hallux Abducto Valgus Deformity
 Distal Metaphyseal Osteotomies in Hallux Abducto Valgus Surgery
Distal Metaphyseal Osteotomies in Hallux Abducto Valgus Surgery
 Trauma to the Nail and Associated Structures
Trauma to the Nail and Associated Structures
 Congenital Deformities
Congenital Deformities
 Osteotomies of the First Metatarsal Shaft in Hallux Abducto Valgus
Osteotomies of the First Metatarsal Shaft in Hallux Abducto Valgus



