9 Arthritis and other joint disorders
ARTHRITIS
The term arthritis is used here to include both inflammatory and degenerative lesions of a joint.1 It implies a diffuse lesion affecting the joint as a whole. It does not include localised mechanical disorders such as loose body formation or tears of the menisci of the knee, which are better designated as internal derangements. Nor should it embrace acute injuries of joints.
Types of arthritis
For convenience the infective types of arthritis, specifically pyogenic and tuberculous arthritis, have been dealt with in Chapter 7 together with the bone infections caused by the same organisms. Although other types of arthritis, particularly rheumatoid arthritis, have a major inflammatory component they have not been shown to be associated with a specific infective organism or virus. They are therefore considered here together with degenerative osteoarthritis and the less common types of arthritis associated with metabolic disturbances such as gout.
The types of non-infective arthritis that are common, taken worldwide, are:
RHEUMATOID ARTHRITIS (Rheumatoid polyarthritis)
Rheumatoid arthritis is a chronic inflammation of joints, often associated with mild constitutional symptoms. It nearly always affects several joints at the same time (polyarthritis). Joint changes of a similar nature also occur in a number of other conditions such as juvenile chronic arthritis (Still’s disease), Reiter’s syndrome, psoriasis, lupus erythematosus, and other connective tissue or collagen diseases.
Cause. The cause is unknown. At present only two possibilities attract serious consideration:
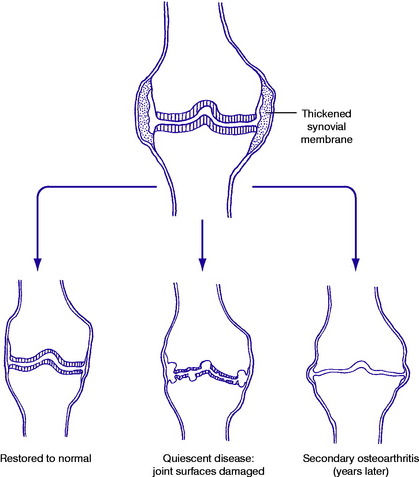
Pathology. The synovial membrane is thickened by chronic inflammatory changes: characteristically it is infiltrated with macrophage-like cells and T-cell lymphocytes (Fig. 9.1). Later the articular cartilage is gradually softened and eroded, and the subchondral bone may also be eroded, characteristically at the joint margins – probably from the action of lytic enzymes and inflammatory mediators produced in the thickened synovial membrane. The eroded surfaces become covered by a soft membrane of inflammatory tissue known as ‘pannus’.
On examination the affected joints are swollen from synovial thickening. The overlying skin is warmer than normal. The range of joint movements is restricted, and movement causes pain, especially at the extremes. These clinical features are often more severe in sero-positive disease than when rheumatoid factor is absent from the serum.
Extra-articular features may include enlargement of lymph nodes, muscle wasting, subcutaneous rheumatoid nodules, and anaemia.
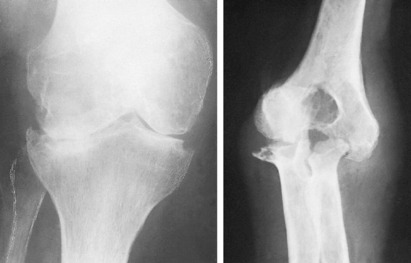
Imaging. Radiographic features: At first there is no alteration from the normal. Later, there is diffuse rarefaction in the area of the joint. Eventually destruction of joint cartilage may lead to narrowing of the cartilage space and, in severe cases, to localised erosion of the bone ends (Fig. 9.2) especially in periarticular sites. Radioisotope bone scanning shows increased uptake of the isotope in the region of affected joints.
A search should always be made for evidence of one of the distinct clinical entities that may be associated with joint changes of a rheumatoid type. The most important of such conditions are:
These conditions are all sero-negative, and they may be associated with ankylosing spondylitis.
Methods of treatment may be classified into the following categories:
Drugs. Drugs used in rheumatoid arthritis fall mainly into the categories of the NSAIDs, and the potent anti-inflammatory agents grouped under the heading of corticosteroids. A logical plan is to use aspirin since it has both analgesic and mild anti-inflammatory properties, but to be effective it may have to be given in fairly large doses. Alternative first-line drugs should probably be chosen from the group of NSAIDs, which includes indometacin, ibuprofen, naproxen, phenoprofen and piroxicam. Due regard must be paid to the risk of side effects: gastric pain is a common complaint with most of these drugs, and more serious complications, such as gastric bleeding, are seen occasionally.
In general, it is wise to avoid repeated injections.
Operation. Operation has an important place in treatment, but each operation must be considered as a component in the overall plan of management and not as a substitute for other measures. Operation may be applicable to the early stages of the disease, or it may be used in the later stages to salvage a joint that has been permanently damaged and remains a source of persistent pain.
Further details are given in the sections on individual joints.








