2 Imaging for orthopaedics
Imaging has now assumed a greater role in the management of patients with orthopaedic disease than ever before. For many years imaging was limited to the use of plain radiographic films which really only gave useful information on bony structures. Over the past 25 years orthopaedics has benefited greatly from newer imaging modalities which are able to give much greater information, not only on the bony structures, but also of the surrounding soft tissues. While plain films remain the mainstay of imaging in trauma, in other orthopaedic conditions they are now less important. Cross-sectional imaging, in particular the use of magnetic resonance imaging (MRI), has now become the most important imaging modality for many orthopaedic conditions. MRI allows detailed identification of the soft-tissue structures in and around joints and for this reason has assumed a very prominent position in imaging of orthopaedic patients.
COMPUTERISED TOMOGRAPHY (CT)
CT is a technique that utilises X-rays, but acquires multiple thin slices axially through the area of interest. With the advances in digital technology modern CT scanners can now acquire this data very rapidly. Current models in use can obtain 16 slices simultaneously, while new machines will be able to acquire 64 and even 256 slices at a time. The result is a stack of very thin radiographic images, usually about 1 mm in thickness. These can be manipulated by the CT computer to generate images in any plane with excellent detail. Typically these images are reformatted into coronal and sagittal planes so that images are similar to looking at AP and lateral radiographs (Fig. 2.1). These images can be acquired in only a few seconds and the reconstructions are also available within a similar short time. Modern scanners can also rapidly reconstruct a three-dimensional model of the scanned area (Fig. 2.2). The commonest role of CT in orthopaedics is assisting in the management of trauma patients with complex fractures. While the fracture is usually easily visualised on plain radiographs, the exact position, number and size of the fracture fragments may be more difficult to identify correctly. This is where CT and its multiplanar capability is of most use in orthopaedic patient management. Typical areas where CT is of most value are in the assessment of fractures in complex anatomical sites, such as the spine, pelvis, tibial plateau and calcaneus. Fracture treatment planning is greatly aided by the multiple views that can be obtained of these complex injuries and in selected cases three-dimensional reconstructions can also add useful information.


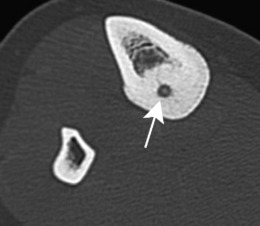
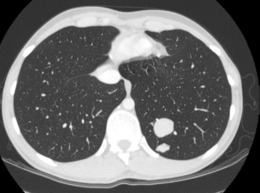
Non-traumatic conditions where CT can be useful are the evaluation of bone- and cartilage-based tumours. Although MRI is the principal method used for the anatomical staging of these tumours, CT may add further useful information regarding the extent of the ossifying or calcified portions of these tumours which an MR scan can underestimate (Fig. 2.3). Another example is osteoid osteoma, where a CT scan provides the diagnostic finding of a very small central sclerotic nidus (Fig. 2.4). A CT scan is also valuable for the full staging of bone and soft-tissue sarcomas, where it is used routinely to detect the presence of lung metastases (Fig. 2.5).
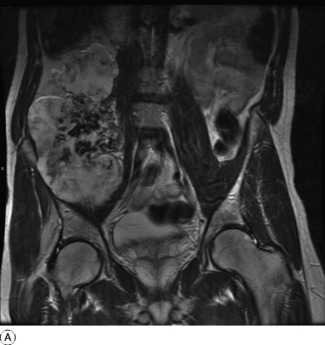
Fig. 2.3 A MRI scan of a very large mass arising from the pelvis and occupying a large part of the abdomen. B A coronal reformatted CT of the same lesion. This shows the bony origin and the bone content of the tumour which is not well seen on the MRI scan.