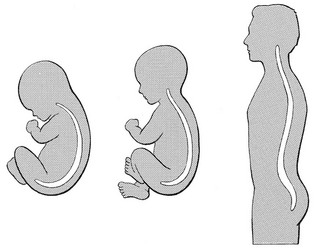
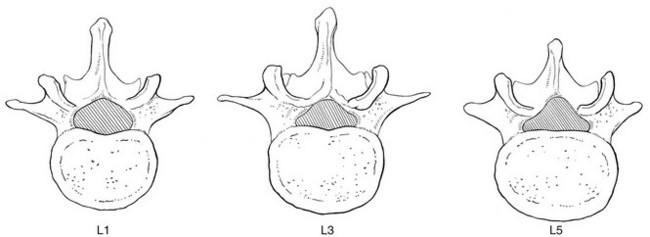
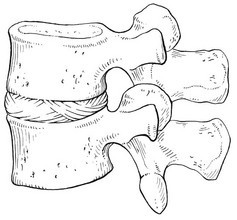
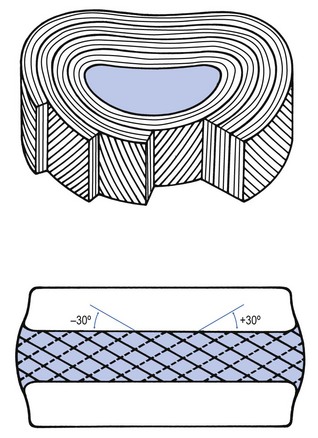
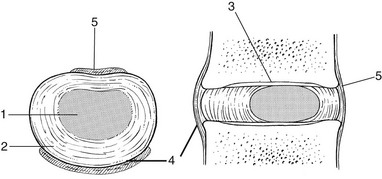
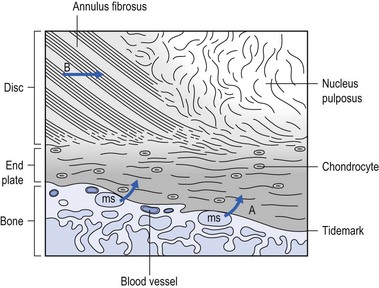
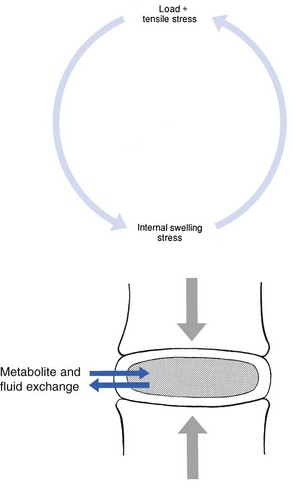
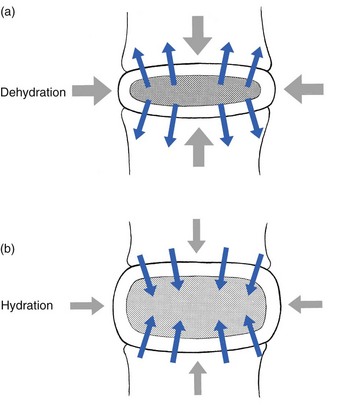
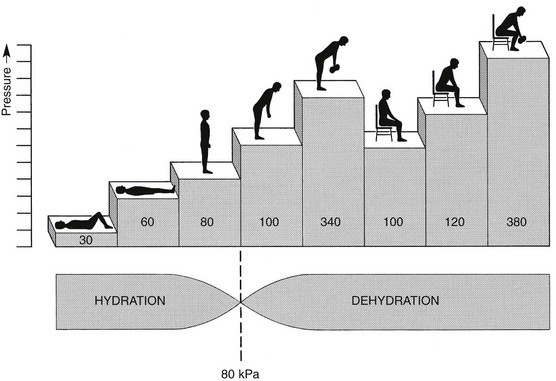
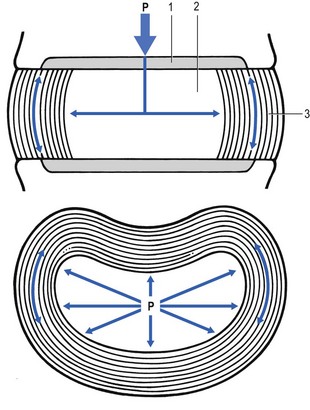
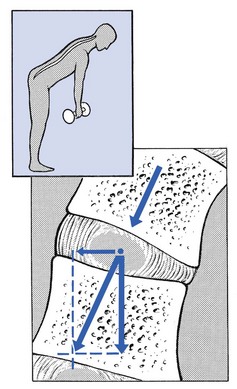
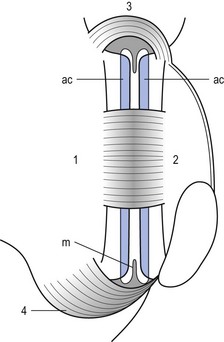
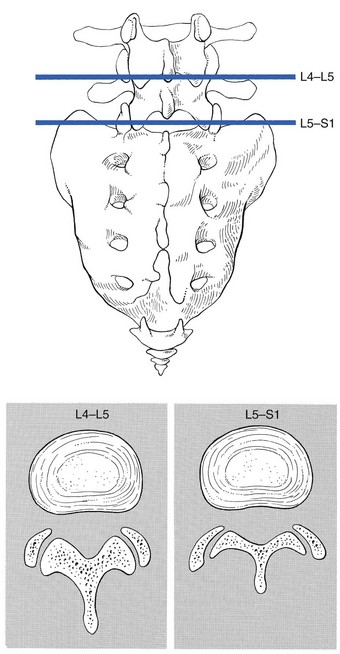
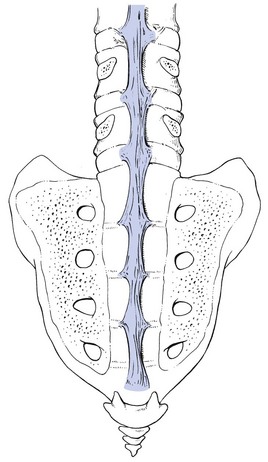
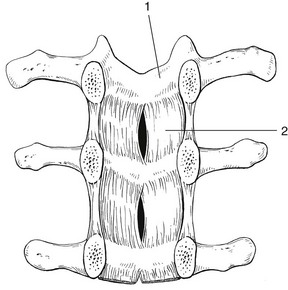
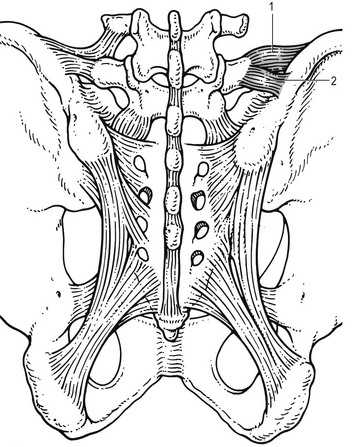
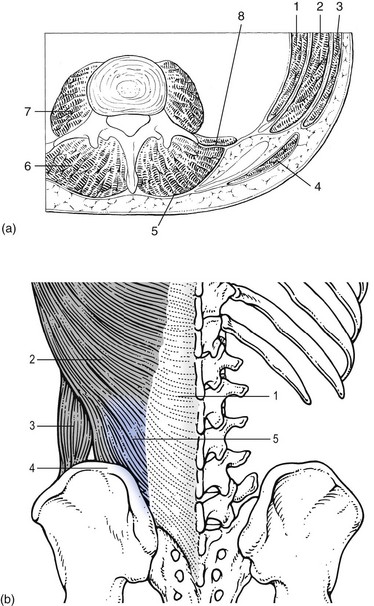
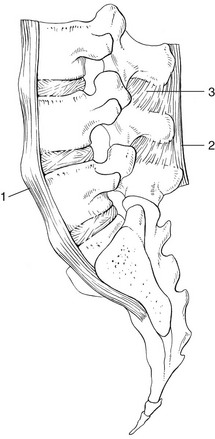
31 The human spine is a self-supporting construction of skeleton, cartilage, ligaments and muscles. Erect, there are four sagittal curves, which are the result of man’s evolution from quadruped to biped. This began in Africa 3 million years ago with Homo australo-pithecus, which had a pelvis strong enough to support an erect posture. After a further 1.5 million years, the definitive erect posture had been adopted – Homo erectus.1 The four curves resulted: cervical lordosis, thoracic kyphosis, lumbar lordosis and sacrococcygeal kyphosis. This S form seems to be a compromise between the static and the dynamic qualities of the spine2; theoretical considerations suggest that the S form is the shape an elastic bar adopts when it is subjected to axial compression.3 The phylogenetic evolution from the large thoracolumbar kyphotic spine of a quadruped into two kyphotic and lordotic curves is also reflected in the spine’s ontogeny. In intrauterine life and during the first 5 months after birth, the spinal curves are absent and there is only one slight kyphosis of the whole spine. At 13 months the lumbar spine is straight, at 3 years some lumbar lordosis is present, and by 8 years the lumbar spine has attained its normal adult posture (Fig. 31.1).4 The development of the erect posture is recent and it seems that, apart from the compensatory lordosis, not much in the way of structural adaptation has taken place. Comparative anatomical evidence suggests that the spine has evolved as a hanging structure between the anterior and the posterior parts of the body. However, during development from quadruped to biped, the function of the spine had to alter completely (Table 31.1); this has serious consequences. In an upright position, the spine is submitted to axial load, which probably leads to the premature disc degeneration from which humans are apt to suffer. In the upright position, the lumbar spine has to resist flexion, whereas the quadruped spine has to resist extension because it is structurally undesirable for a ‘bridge’ to sag in the middle. The change to an upright position, however, has not yet been followed by anatomical adaptation, and the human spine has an anatomy that more readily withstands extension than flexion: the anterior part of the annulus fibrosus is stronger and thicker than the posterior, and the anterior longitudinal ligament is almost twice as thick and broad as the posterior.5 Table 31.1 Comparison of the quadruped and biped lumbar spines Each vertebral body is more or less a cylinder with a thin cortical shell which surrounds cancellous bone. From L1 to L5, the posterior aspect changes from slightly concave to slightly convex, and the diameter of the cylinder increases gradually because of the increasing loads each body has to carry. At the upper and lower surfaces, two distinct areas can be seen: each is a peripheral ring of compact bone – surrounding and slightly above the level of the flat and rough central zone – which originates from the apophysis and fuses with the vertebral body at the age of about 16. The central zone – the bony endplate – shows many perforations, through which blood vessels can reach the disc. A layer of cartilage covers this central zone, which is limited by the peripheral ring. This is the cartilaginous endplate, forming the transition between the cortical bone and the rest of the intervertebral disc. A sagittal cut through the vertebral body shows the endplates to be slightly concave, which consequently gives the disc a convex form.6 The two pedicles originate posteriorly and attach to the cranial half of the body. Together with the broad and flat lamina, they form the vertebral arch. From L1 to L5, the pedicles become shorter and broader, and are more lateral. This narrows the anteroposterior diameter and widens the transverse diameter of the vertebral canal from above downwards. Together with the increasing convexity of the posterior aspect of the vertebral body, these changes in the position of the pedicles alter the shape of the normal bony spinal canal from an ellipse at L1 to a triangle at L3 and more or less a trefoil at L5 (Fig. 31.2). The part of the lamina between the superior and inferior articular processes is called the ‘pars interlaminaris’. It runs obliquely from the lateral border of the lamina to its upper medial border. This portion of the lamina is subjected to considerable bending forces, as it lies at the junction between the vertically oriented lamina and the horizontally oriented pedicle. This ‘interlaminar part’ will therefore be susceptible to fatigue fractures or stress fractures (spondylolysis) (see Ch. 39).7 Two adjacent vertebral bodies are linked by an intervertebral disc. Together with the corresponding facet joints, they form the ‘functional unit of Junghans’ (Fig. 31.3).8 An upper and a lower cartilaginous endplate (each about 0.6–1 mm thick) cover the superior and inferior aspects of the disc. They are plates of cartilage that bind the disc to their respective vertebral bodies. Each endplate covers almost the entire surface of the adjacent vertebral body; only a narrow rim of bone, called the ring apophysis, around the perimeter of the vertebral body is left uncovered by cartilage. That portion of the vertebral body to which the cartilaginous endplate is applied is referred to as the vertebral endplate. The endplate covers the nucleus pulposus in its entirety; peripherally it fails to cover the entire extent of the annulus fibrosus.9 The collagen fibrils of the inner lamellae of the annulus enter the endplate and merge with it, resulting in all aspects of the nucleus being enclosed by a fibrous capsule.10 The endplate permits diffusion and provides the main source of nutrition for the disc.11,12 Up to the age of 8 years, the cartilaginous endplates are penetrated by blood vessels which pass into the peripheral layers of nucleus and annulus. Thereafter, the disc’s nutrition is achieved by diffusion through the endplate. The hyaline endplate is also the last part of the disc to wear through during severe disc degeneration.13 This is made up of 15–25 concentric fibrocartilaginous sheets or ‘lamellae’ (Fig. 31.4), each formed by parallel fibres, running obliquely at a 30° angle between the vertebral bodies.14 Because the fibres of two consecutive layers are oriented in opposite directions, they cross each other at an angle of approximately 120°.15 This arrangement of the annular fibres gives the normal disc great strength against shearing and rotational stresses,16 while angular movements remain perfectly possible.17,18 The outermost fibres are attached directly to bone, around the ring apophysis, and for that reason they are referred to as the ligamentous portion of the annulus fibrosus. The inner third merges with the cartilaginous endplate and is referred to as the capsular portion of the annulus fibrosus (Fig. 31.5). This consists of a gelatinous substance, made of a meshwork of collagen fibrils suspended in a mucoprotein base which contains mucopolysaccharides and water.19 With advancing age, the amount of mucopolysaccharides diminishes, as does that of the water they bind. A young nucleus is 85% water, whereas it is only 65% water in the elderly.20 These biological changes are mirrored in the macroscopic aspects of the nucleus. In the second and third decades the nucleus is clear, firm and gelatinous but subsequently it becomes drier and more friable. In the elderly, the nucleus has the texture of thickened cream cheese, and is dry, brownish and friable. At birth the nucleus pulposus occupies the centre of the intervertebral space. As the anterior part of the vertebral body grows faster than the posterior part, the nucleus comes to lie more posteriorly. Consequently, the anterior part of the annulus will have thicker and stronger fibres,21 which means that the annulus gives better protection against anterior than posterior displacements of the nucleus; this is disadvantageous with respect to the contiguous nerve roots and dura. Cartilage is devoid of nerves and it has been conventional to draw the same conclusions about the disc. However, over the last few decades, there has been a great deal of research on the possibility that there is some innervation. The presence of free nerve endings has been demonstrated as far as one-third of the way into cadaveric annuli fibrosi,22 and as far as halfway into annuli fibrosi obtained during posterior fusion operations.23 Other research has shown a few nervous elements in the periphery of the annulus fibrosus.24,25 More recent studies have demonstrated mechanoreceptors to be present in the outer two or three lamellae of the human intervertebral disc and the anterior longitudinal ligament.26 Although the presence of substance P – generally accepted as an important nociceptive neurotransmitter – has so far not been demonstrated in human intervertebral discs,27 other neuropeptides have.28,29 The exact relationship between the existence of small nerve endings in the outer layers of the disc and back pain therefore still remains controversial. The lack of blood supply to the intervertebral disc has been shown by microangiographic studies.30 There is some vascularization of the vertebral borders of the disc in children but by the age of 8 years all cartilaginous penetration by blood vessels has disappeared. Vascular buds in the bony endplate remain during adulthood as a vascular bed under the cartilaginous endplate, and diffusion from these through the endplates remains the main nutritional pathway for the disc during adult life,31,32 although some nutrition via contact with the intimate anterior and posterior longitudinal ligaments is also possible (Fig. 31.6).33 The disc is thus the largest non-vascular structure in the body, which causes difficulties in healing and regeneration after damage. The main structural components of the intervertebral disc are collagen, proteoglycans (PGs) and water. The water is not free but is bound by the PGs,34 which, because of their pronounced osmotic properties, maintain the hydration and turgor of the disc. The proportion of the three constituents varies across the disc. Fluid and PG concentrations are highest in the nucleus and lowest in the annulus, whereas the reverse is true for collagen. Proteoglycans are complex chemical structures, existing as monomer subunits and aggregates. The former are made up of a central protein molecule with an attached long-chain glucosaminoglycan; the latter consist of monomers, attached to a long hyaluronic acid filament (see Ch. 3). The synthesis of PGs is performed by the cartilage cells and is a continuous process, demanding a well-balanced metabolism.35 For its nutrition, the disc, devoid as it is of any penetrating vascular structure, depends entirely on diffusion through the central portion of the endplates and the outer annulus (see Fig. 31.6).11,36 Consequently, the disc is vulnerable and changes in its composition are inevitable as age advances. Although the total collagen content remains fairly constant during adult life,37 the PG concentration falls.38,39 The result is that the osmotic properties and the turgor of the disc will also decline as age advances (see p. 438).40 Proteoglycans play a key role in the osmotic system of the intervertebral joint, which incorporates the nucleus, annulus and cartilaginous endplates, and also the cancellous bone of the vertebrae. Two compartments – nucleus and paravertebral tissues – are separated by the semipermeable barrier formed by the cartilaginous endplate and the annulus fibrosus, which permits the transport of small molecules only: water, ions and substances of low molecular weight. Diffusion tests with dye demonstrate that only substances with a molecular weight under 400 can pass the disc tissue barrier.41 The PGs of the inner compartment take up water, until the hydrostatic pressure that results is in balance with the physical tension that arises from the tensile forces of the annulus and the loads applied by muscles, ligaments and gravity (Fig. 31.7). At this point, there is no net fluid loss or gain. If the external stress is increased – say, by an increase in load – the balance will be disturbed and fluid is expressed from the nucleus (Fig. 31.8a). This loss of fluid has two consequences: tensile stress in the collagen network falls and the concentration of PGs in the nucleus and thus the osmotic pressure rise. In other words, loss of fluid increases the internal swelling pressure, until the latter has risen to the physical stress and a new balance is achieved.43 The reverse happens when the external load decreases: the internal osmotic pressure is momentarily higher than the external load and fluid is attracted (Fig. 31.8b). The concentration of PGs and the swelling pressure decrease until external and internal pressures again reach an equilibrium. Using diffusion techniques with dye and with radioactive substances, Krämer was able to show that in normal non-degenerated discs there is an extravasation of fluid when a load of more than 80 kPa is applied. Absorption takes place when the load is lower than 80 kPa.45 From 1966 on, Nachemson and co-workers demonstrated the relationship between body posture and intradiscal pressure by intravital recordings.46–51 They demonstrated that the pressure in an L3 disc of a healthy individual, weighing 70 kg, is 30 kPa in a supine lying position. Standing and walking around sets up a pressure between 70 and 85 kPa, whereas sitting raises the pressure to 100 kPa and slightly bending forwards to 120 kPa. Lifting a 20 kg object with a bent back and straight legs increases the intradiscal pressure to a surprising 340 kPa. These findings suggest the dehydration–hydration point, found by Krämer to be around the standing and walking position (Fig. 31.9). The supine position causes hydration of the disc, whereas sitting, bending or lifting squeezes fluid out of the disc. Since the transport processes in the disc depend largely on fluid flow, continuous change in intradiscal pressure could be of utmost importance for the nutrition of the disc.53 Load and de-load acts as a pump, and transports water and metabolites from and to the intervertebral disc.54 In order to protect discs against early degeneration, it is therefore important to keep the intradiscal pressure as low as possible during daily activities. This can be achieved by adopting a slight lordosis at the lumbar spine which protects the disc against excessive pressure. Also, regular changes in position continuously alter the intradiscal pressure, so causing a nutritional fluid flow to and from the disc.55 The prophylactic measures derived from these findings will be discussed in the section on back schools (see p. 582). The fibroelastic annulus provides the disc with hydraulic properties and provides resistance to tensile forces. Retained by this fibroelastic mesh, the nucleus pulposus acts like a fluid-filled balloon. During load, it distributes the axial pressure equally over the cartilage plates and the annulus fibrosus (Fig. 31.10). The annular fibres are under a constant slight stretch, because of the turgor of the nucleus. McNab56 compares the annulus with a coiled spring that pulls the vertebral bodies together against the turgor of the nucleus. If the load is axial and symmetrical, the nucleus pulposus distributes the force to all sides and therefore perpendicularly on the stretched annular fibres. In this position the disc is very strong and, during high compressive loads, outward herniation of the nucleus is not seen but there is a collapse of the cartilaginous endplates.57,58 Asymmetrical loading, however, simultaneously involves tension, compression and shear stresses at different locations in the disc. Bending results in a tensile stress on the convex side and a compressive stress on the concave side: that under tension stretches, while that under compression bulges.59,60 Tensile stresses on the convex side are increased by the migration of the nucleus. During such asymmetrical loading, the nucleus pulposus is pushed away from the area of compression, following the simple mathematical parallelogram of forces (Fig. 31.11). This means that, in bending forwards, the nucleus will move posteriorly, and therefore greater stress will fall on the posterior annular fibres, which are already subjected to a strong tensile stress. The posterior migration of the nucleus pulposus in bending has been demonstrated experimentally by putting a metal pin in the nucleus pulposus.61 On continuous forward bending, the nucleus migrated backwards at a speed of 0.6 mm/min during the first 3 minutes and this continued very slowly during the next hour. After bending ceased, the nucleus regained its original position only very slowly. These findings have been confirmed by discography62 and by magnetic resonance imaging (MRI) studies.63–65 Biomechanical studies, conducted in vitro, have also demonstrated that the normal nucleus moves posteriorly in kyphosis and anteriorly in lordosis.66–68 Several anatomical, biochemical and biomechanical properties make the posterior aspect of the disc the most critical and vulnerable part of the whole intervertebral joint.69,70 • The posterior annular fibres are sparser and thinner than the anterior. • Because the area available for diffusion is smaller posteriorly than anteriorly, the posterior part of the nuclear–annular boundary receives less nutrition and again the posterior part of the disc is the most strained part.71 • The posterior longitudinal ligament affords only weak reinforcement, whereas the anterior fibres are strengthened by the powerful anterior longitudinal ligament. • Because of the special mechanical arrangements of the annular fibres, the tangential tensile strain on the posterior annular fibres is 4–5 times the applied external load.72 In order to prevent early degeneration and internal derangement, the erect body has developed only one adequate defence system: namely, a slightly lordotic lumbar posture. Cyriax was the first clinician to point out the importance of the lumbar lordosis. Long before biomechanical experiments, such as those of Nachemson, and purely on clinical findings, he demonstrated the importance of correct posture in the avoidance of backache and sciatica.73 This is the physiological lumbar lordosis, which diminishes the intradiscal pressures and protects the disc against backward displacements of the nucleus pulposus. ‘Keep your back hollow’ is still the best advice against recurrent discogenic backache, even more so in recent decades because of the more sedentary jobs many people have. A sitting position not only increases the intradiscal pressure but also forces the lumbar spine into kyphosis by a backwards inclination of the sitting pelvis.74 Increased sedentary work is probably one of the reasons for the rising rate of lumbar syndromes. The joints between the lower and upper articular processes are called zygapophyseal joints, apophyseal joints or ‘facet’ joints. They are true synovial joints, comprised of cartilaginous articular surfaces, synovial fluid, synovial tissue and a joint capsule (Fig. 31.12). The superior articular surface is slightly concave and faces medially and posteriorly. The convex inferior articular surface points laterally and slightly anteriorly. In general terms, there is a change from a relatively sagittal orientation at L1–L3, to a more coronal orientation at L5 and S1 (Fig. 31.13).75,76 Unlike the disc, the facet joints normally do not bear weight and during normal loads they are not subjected to compression strain.72 In degenerative fragmentation of the disc, however, intervertebral height diminishes and the articular surfaces are subjected to abnormal loading, setting up spondylarthrosis.77 The main function of the facet joints is to guide lumbar movements and keep the vertebrae in line during flexion–extension and lateral flexion. Because of the more sagittal slope of the articular surfaces, very little rotation takes place at the four upper lumbar levels. More distally, at the lumbosacral level, the joint line has a more coronal plane, which makes rotational movements potentially possible, but these are limited by the iliolumbar ligaments (see p. 424).78 The total range of rotation in the lumbar spine is therefore very limited, although not completely zero.79 The capsule of the joints is well developed and thick and elastic at the dorsal, superior and inferior aspects. At rest, the fibres run slightly diagonally from lateral–caudal to medial–cranial. As the articular excursion is about 0.5 cm at each level, the capsule must have a considerable laxity to follow the points of insertion during flexion. It therefore possesses capsular recesses of varying size, at the superior and inferior poles of the joint, which gives the joint the appearance of a dumb-bell during arthrographic examinations.80 In extension the posterior capsule can become pinched between the apex of the inferior facet and the lamina below. In order to prevent this, some fibres of the multifidus blend with the posterior capsular fibres and keep the capsule taut.81 The ventral aspect of the capsule is an extension of the ligamentum flavum. It is very thin82 and may rupture during intra-articular injections.83 During flexion, the inferior articular process slides upwards on the superior articular process. The lower part of the latter loses contact and becomes exposed. Similarly, the lower part of the inferior articular process becomes exposed ventrally. In order to protect these exposed surfaces, and to maintain a film of synovial fluid over the articular cartilages, the facet joints are endowed with small intra-articular ‘meniscoids’.84–86 These small fibro-adipose crescent wedges have a base attached to the joint capsule and an apex that projects into the capsular pouches.87 Stretching of the capsule during flexion makes them disappear. Some believe that these fibro-adipose enlargements could become pinched between the articular surfaces, constituting a probable source of backache.88–91 The facet joints are innervated by fibres of the medial branch of the dorsal root. The same nerve supplies the inferior aspect of the capsule and the superior aspect of the joint below.92 The broad, thick anterior longitudinal ligament (Fig. 31.14) originates from the anterior and basilar aspect of the occiput and ends at the upper and anterior part of the sacrum. It consists of fibres of different lengths: some extend over 4–5 vertebral bodies; the short fibres attach firmly to the fibres of the outermost annular layers and the periosteum of two adjacent vertebrae. Fig 31.14 Anterior longitudinal (1) and supraspinous and interspinous ligaments (2 and 3, respectively). The posterior longitudinal ligament (Fig. 31.15) is smaller and thinner than its anterior counterpart: 1.4 cm wide (versus 2 cm in the anterior ligament) and 1.3 mm thick (versus 2 mm). This is another fact in favour of the theory that the lumbar spine was originally designed to be a horizontal hanging structure: to withstand extension strains, the back had to be stronger anteriorly than posteriorly.5 The posterior longitudinal ligament is narrow at the level of the vertebral bodies, and gives lateral expansions to the annulus fibrosus at the level of the disc, which bestow on it a denticulated appearance.93 Although the posterior ligament is rather narrow, it is important in preventing disc protrusion.94 Its resistance is the main factor in restricting posterior prolapse and accounts for the regular occurrence of spontaneous reduction in lumbago. This characteristic is also exploited in manipulative reduction, when a small central disc displacement is moved anteriorly when the ligament is tightened. The fact that the ligament occupies only the midline of the vertebral column is one of the predetermining factors in the progression of sciatica: as a central protrusion enlarges, it tends to move in the direction of least resistance – lateral to the ligament. Once free from ligamentous resistance, it further enlarges and starts to compress the nerve root. This anatomical evolution is mirrored by the change in the clinical picture: a central backache is replaced by a unilateral sciatica. The ligamentum flavum (Fig. 31.16) connects two consecutive laminae and has a very elastic structure with an elastin content of more than 80%.82 The lateral extensions form the anterior capsule of the facet joints and run further laterally to connect the posterior and inferior borders of the pedicle above with the posterior and superior borders of the pedicle below. These lateral fibres form a portion of the foraminal ring and the lateral recess.95,96 The interspinous ligament (see Fig. 31.14) lies deeply between two consecutive spinal processes. Unlike the longitudinal ligaments, it is not a continuous fibrous band but consists of loose tissue,97 with the fibres running obliquely from posterosuperior to anteroinferior.98 This particular direction may give the ligament a function over a larger range of intervertebral motion than if the fibres were vertical.99 The ligament is also bifid, which allows the fibres to buckle laterally to both sides when the spinous processes approach each other during extension.97 The supraspinous ligament is broad, thick and cord-like. It joins the tips of two adjacent spinous processes, and merges with the insertions of the lumbodorsal muscles. Some authors consider the supraspinous ligament as not being a true ligament, as it seems to consist largely of tendinous fibres, derived from the back muscles.100 The effect of the supraspinous ligaments on the stability of the lumbar spine should not be underestimated.101 Because the ligament is positioned further away from the axis of rotation and due to its attachments to the thoracolumbar fascia,102 it will have more effect in resisting flexion than all the other dorsal ligaments. Pearcy103 showed that the distance between the tips of the spinous processes increases during full flexion by 360% at L3–L4 and 129% at L5–S1. By contrast, the posterior longitudinal ligament only increases by 55% at L3–L4 and 34% at L5–S1. This demonstrates the limiting effect of the ligament on the increasing posterior disc height during stooping. The importance of a strong supraspinous ligament in the prophylaxis of recurrent disc protrusions will be discussed later. The iliolumbar ligaments (Fig. 31.17) are thought to be related to the upright posture.104 They do not exist at birth but develop gradually from the epimysium of the quadratus lumborum muscle in the first decade of life to attain full differentiation only in the second decade.105 The ligament consists of an anterior and a posterior part.106–108 The anterior band of the iliolumbar ligament is a well-developed, broad band. Its fibres originate from the anterior–inferior part of the L5 transverse process from as far medially as the body of the L5 vertebra to the tip of the transverse process, and expand as a wide fan before inserting on the anterior part of the iliac tuberosity. The posterior band of the iliolumbar ligament originates from the apex of the L5 transverse process and is thinner than the anterior. It inserts on the iliac crest, behind the origin of the quadratus lumborum.108 The iliolumbar ligaments play an important role in the stability of the lumbosacral junction by restricting both side flexion and rotational movement at the L5–S1 joint and forward sliding of L5 on the sacrum.104,109,110 One clinical consequence of this is that posterolateral disc protrusions at the L5–S1 level will not be followed by large lateral flexions of L5 on the sacrum. Marked adaptive deformity will therefore be absent here. Consequently, a large lateral tilt in a patient with acute backache means a displacement at L3–L4 or L4–L5, since these intervertebral joints can open up more easily. Also, stabilization of the lumbosacral junction by the strong iliolumbar ligaments may explain the fact that L5–S1 pars defects are more stable than L4–L5 lesions (see spondylolisthesis, Ch. 58).111,112 The spine is unstable without the support of the muscles that power the trunk and position the spinal segments.113 Back muscles can be divided in four functional groups: flexors, extensors, lateral flexors and rotators (Fig. 31.18). The extensors are arranged in three layers: the most superficial is the strong erector spinae or sacrospinalis muscle. Its origin is in the erector spinae aponeurosis, a broad sheet of tendinous fibres attached to the iliac crest, the median and lateral sacral crests and the spinous processes of the sacrum and lumbar spine.114 The middle layer is the multifidus. The fibres of the multifidus are centred on each of the lumbar spinous processes. From each spinal process, fibres radiate inferiorly to insert on the lamina, one, two or three levels below. The arrangement of the fibres is such that it pulls downwards on each spinal process, thereby causing the vertebra of origin to extend.115
Applied anatomy of the lumbar spine

Human posture
Quadruped
Biped
Structure
Horizontal
Vertical
Load
Horizontal
Axial
Curve
Slight kyphosis
Lordosis
Strength
Against extension
Against flexion
Strong structures
Anterior
(Posterior?)
Vertebrae
Vertebral bodies
Pedicles
Laminae
Intervertebral discs
Endplates
Annulus fibrosus
Nucleus pulposus
Behaviour of the disc
The disc as an osmotic system
Influence of the external load on hydration of the disc
Biomechanical properties of the disc
The weak zone of the disc
Facet joints
Ligaments
Muscles and fasciae
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Musculoskeletal Key
Fastest Musculoskeletal Insight Engine