1. How did the injury occur?
a. Was there contact with another athlete?
b. Was there a fixed position of the foot and rotation or twisting movement?
2. Were you able to continue to compete?
3. Was there significant swelling directly after the injury?
4. Have there been previous injuries to the knee?
participating in cutting and contact sports. The typical presentation is a young athlete who has a decelerating, twisting injury. Approximately two-thirds of ACL injuries occur by noncontact mechanisms (10). The patient will often report a “pop” and the inability to return to the field. A large amount of swelling due to hemarthrosis is expected. The presentation is less dramatic in athletes who have had a prior partial tear of the ACL.
 FIGURE 80.1. MRI demonstrating midsubstance ACL tear. |
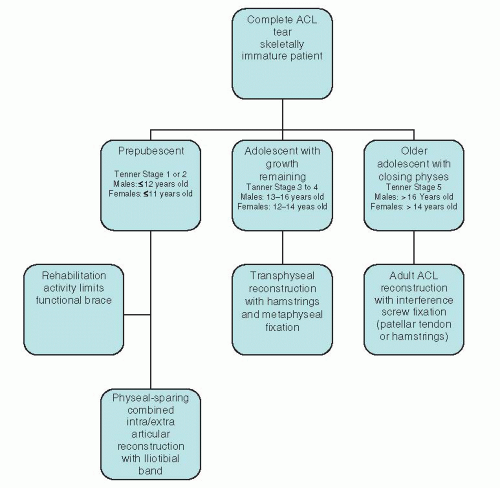 FIGURE 80.2. Algorithm for management of complete ACL injuries in skeletally immature patients. |
Table 80.1 Tanner staging classification of secondary sexual characteristics | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Related posts:
 Acromioclavicular Separations: Arthroscopic Reconstruction of The Acromioclavicular Joint
Multidirectional and Posterior Shoulder Instability
The Stiff Shoulder: Planning and Treatment Options
Arthroscopic Suprascapular Nerve Release
Arthroscopic Management of Lateral Epicondylitis
Clinical Approach to Articular Cartilage Pathology
Acromioclavicular Separations: Arthroscopic Reconstruction of The Acromioclavicular Joint
Multidirectional and Posterior Shoulder Instability
The Stiff Shoulder: Planning and Treatment Options
Arthroscopic Suprascapular Nerve Release
Arthroscopic Management of Lateral Epicondylitis
Clinical Approach to Articular Cartilage Pathology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


