Anconeus Arthroplasty
Bernard F. Morrey
Alberto G. Schneeberger
INTRODUCTION
The management of posttraumatic proximal radiohumeral and radioulnar dysfunction, pain, or instability is a challenging problem without well-documented solutions. The unreliability or unsuitability of prosthetic replacement and lack of an alternate solution have prompted the development of a proximally based soft tissue rotational arthroplasty procedure employing the anconeus muscle. The attractiveness of this procedure is that the muscle is innervated and vascularized from distinct vascular pedicles originating from the recurrent posterior interosseous artery and from the medial collateral artery (1). This allows the entire muscle to be mobilized, leaving it attached to the triceps fascial expansion, preserving its viability. Cadaver dissections have demonstrated a mean length of approximately 9 to 10 cm and a width of about 3 cm (2) (Fig. 30-1), sufficient to allow several variations of interposition procedures. Furthermore, the absence of this muscle from its anatomic location does not result in any measurable dysfunction or morbidity from a recovery or functional perspective.
The procedure was first performed approximately 10 years ago. Although there are few data regarding the long-term value of the method (2), it is included here for the purpose of introducing the concept as a potential but not necessarily a proven or definitive solution for difficult reconstructive problems for which reliable alternatives do not exist.
INDICATIONS/CONTRAINDICATIONS
In general, this technique is employed in instances when proximal radioulnar or radiohumeral dysfunction occurs following trauma. The three primary indications for the procedure are
Radiohumeral impingement in which the interposition is principally directed at the proximal radiocapitellar articulation
Proximal radioulnar impingement with or without radiohumeral impingement
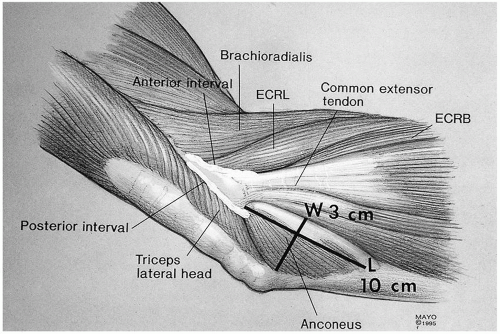 FIGURE 30-1 The mean dimensions of the anconeus muscle are 9 to 10 cm in length and 3 to 3.5 cm in width at its fascial attachment to the triceps. |
The primary contraindication to this procedure is an absent or devitalized anconeus muscle. A condition requiring a procedure that resists high axial load along the radius would also rule out use of an anconeus arthroplasty. Lastly, a deficient lateral ulnar collateral ligament that cannot be reconstructed prohibits use of this procedure.
SURGERY
Several variations of the interposition have been used and are classified as follows: type I, radiohumeral “roll-up” interposition; type II, radiohumeral/radioulnar interposition; and type III, proximal radial “wrap” (Fig. 30-2). The specific pathoanatomy determines which of the three types of interposition is appropriate. The method of harvest is common for all these applications.
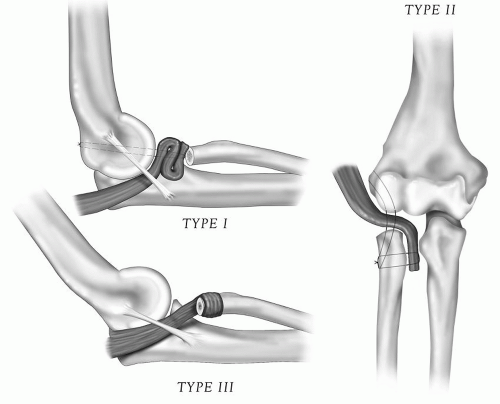 FIGURE 30-2 Variations of anconeus rotation/interposition arthroplasty: type I, radiohumeral; type II, radiohumeral/radioulnar; and type III, radial “wrap.” |
Anconeus Harvest
The patient is placed supine with the forearm brought across the chest. Any previous incision in the region is entered, or a Kocher-type skin incision is made (Fig. 30-3). The interval between the anconeus and extensor carpi ulnaris is entered and expanded to expose the anconeus muscle (Fig. 30-4). The dissection must be carried distally approximately 10 cm from the lateral epicondyle to expose the distalmost aspect of this muscle insertion. The tip of the anconeus is identified. The muscle is then reflected from the ulna and from the common retinaculum (Fig. 30-5). The dissection is carried proximal to the point of origin from the fascial expansion and attachment to the triceps, retaining its innervation and vascularity (Fig. 30-6).
The lateral joint is entered anterior to the collateral ligament, and the relevant pathology is identified. The posterior margin of the ligament is then identified. As in all instances, the transposed muscle is placed under the lateral ulnar collateral ligament (Fig. 30-7).
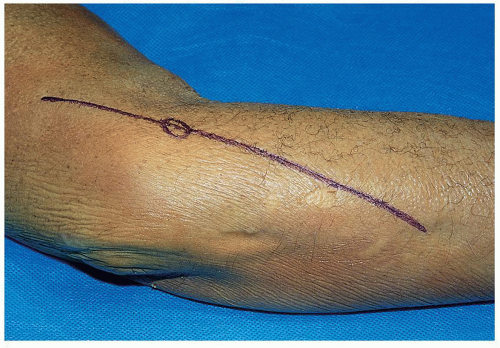 FIGURE 30-3 A Kocher skin incision is made. |
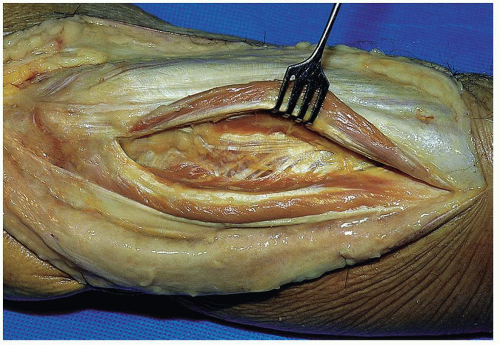 FIGURE 30-4 The interval between the anconeus and extensor carpi ulnaris is identified and developed. |
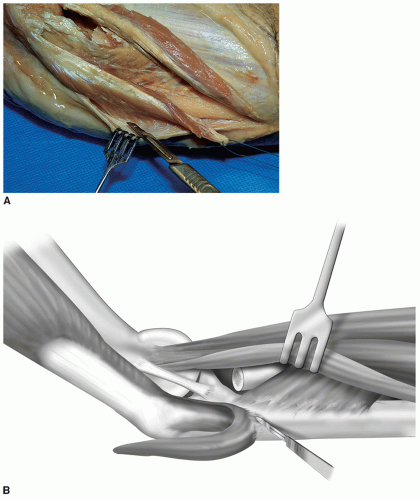 FIGURE 30-5 A,B: The distal aspect of the anconeus is isolated, and the muscle is elevated from its bed and from the forearm fascia. |
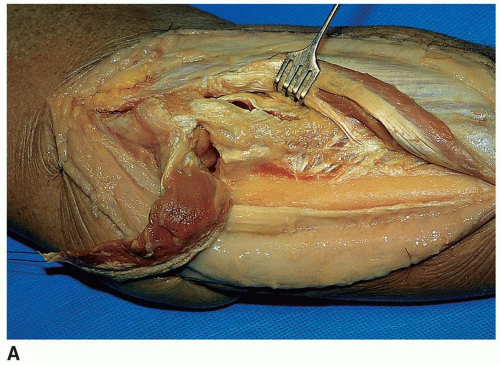 FIGURE 30-6 A,B: The anconeus is reflected proximally on its pedicle attachment to the triceps. |
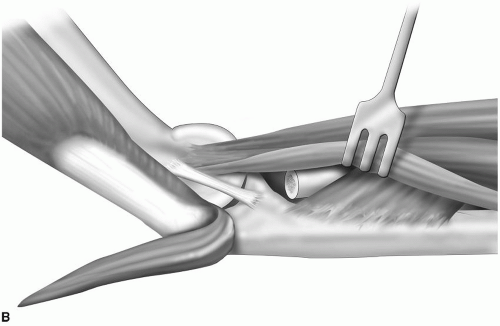 FIGURE 30-6 (Continued) |
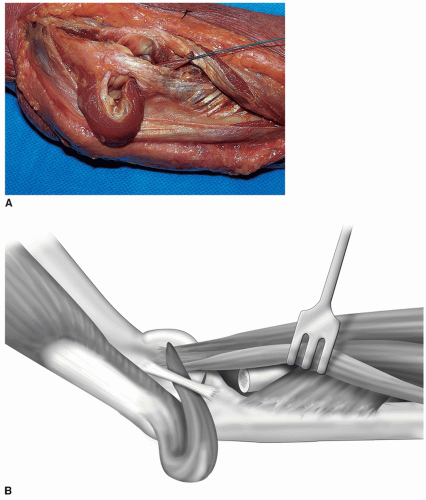 FIGURE 30-7 A,B: In all instances, the muscle is inserted into the joint under the lateral ulnar collateral ligament. |
Type I: Interposition at the Radiohumeral Joint
The integrity of the lateral collateral ligament is assessed. If this is inadequate, it is reconstructed as described in Chapter 15




Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
