Surgical Technique for Capitellar Replacement
Bernard F. Morrey*
*Dr Morrey is the designer of this implant; Small Bone Innovations.
INTRODUCTION
Disease of the ulnohumeral joint is not very common; however, when the primary problem is that of the capitellum, options for intervention are limited. In primary osteoarthritis, radial head resection has been carried out (1). In the past, the author has used capitellar interposition with cutis or allograft material for isolated capitellar pathology. In some instances, an anconeus arthroplasty may be an appropriate reconstruction option for disease of the joint (2). If a need exists to reestablish a capitellar articular surface, replacement might be considered.
INDICATIONS
Instances in which the capitellum has been involved with primary degenerative arthrosis (3,4) or trauma, with or without involvement of the radial head (Fig. 33-1) when capitellar articular restoration is required to control pain or restore stability of the radiohumeral joint (4).
Note: Use of the capitellar replacement without a radial head replacement is considered an offlabel use since the FDA approval was for the replacement of both the radial head and the capitellum. However, if the radial head is normal, there is no reason to replace the radial head, and it is left intact.
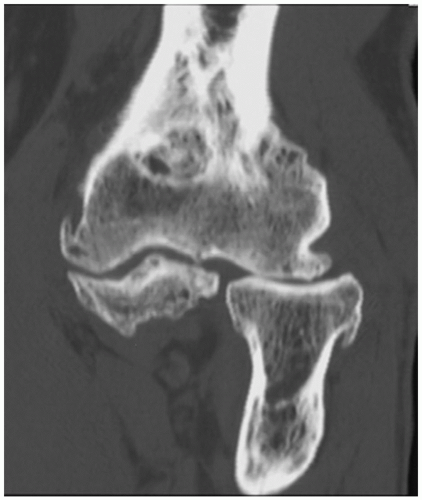 FIGURE 33-1 Primary degenerative arthritis often involves the radiohumeral joint more extensively than the ulnohumeral joint. |
CONTRAINDICATIONS
Except for the loss of capitellar bone stock, the capitellum should not be replaced concurrent with a radial head implant if the host articular surface would appear to possibly tolerate the radial head articulation.
TECHNIQUE
Position
The patient is placed under a general or regional anesthesia.
The extremity is prepped and draped in the usual fashion.
The author prefers a nonsterile tourniquet and to perform the procedure with the arm brought across the chest.
Exposure
A classic Kocher-type skin incision is made entering the interval between the anconeus and extensor carpi ulnaris. The interval is opened and the extensor carpi ulnaris is reflected from the epicondyle, and the anconeus is reflected dorsally along with its humeral origin. This allows identity of the lateral capsule. The joint is entered by a longitudinal incision just anterior to the lateral ulnar collateral ligament.
The humeral origin of the lateral ulnar collateral ligament is reflected dorsally, and the anterior capsule is released from its anterior lateral attachment (Fig. 33-2). This provides an adequate and generous exposure of the lateral ulnohumeral joint.
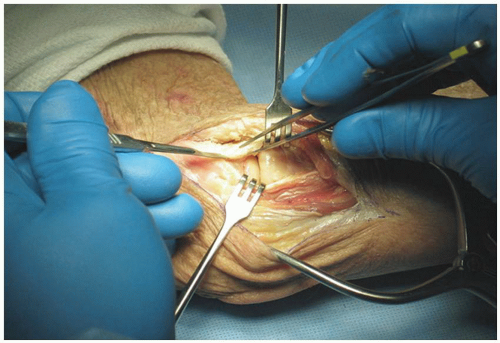 FIGURE 33-2 Exposure for a capitellar replacement involves removing a portion of the attachment of the lateral ulnar collateral ligament. In some instances, if the radial head is not to be replaced, the entire ligament must be released. |
Note: The extent to which the lateral collateral ligament need be released is a function of the pathology and status of the radial head. If the radial head is to be replaced, it is removed first. Since this facilitates the procedure, it may not be necessary to completely release the lateral ulnar collateral ligament.
Identifying the Axis of Rotation
The key to capitellar replacement is to accurately identify the axis of rotation. The tubercle of the lateral epicondyle is identified as this is the origin of the axis. The correct orientation of the axis is achieved by placing the alignment guide over the medial epicondyle. This identifies the axis of flexion of the elbow joint, and a K-wire is placed through the guide in order to replicate this axis with a 0.062 K-wire that fits through the drill guide.
Note: Confirmation of accurate placement of this axis pin may be obtained with fluoroscopy.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


