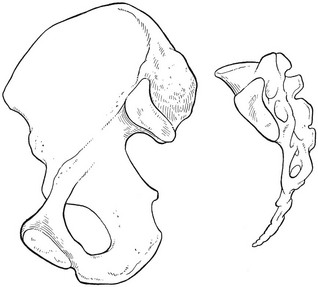
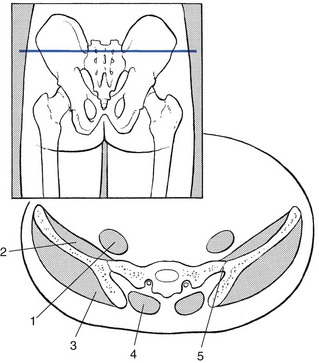
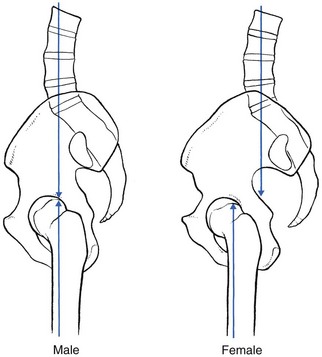
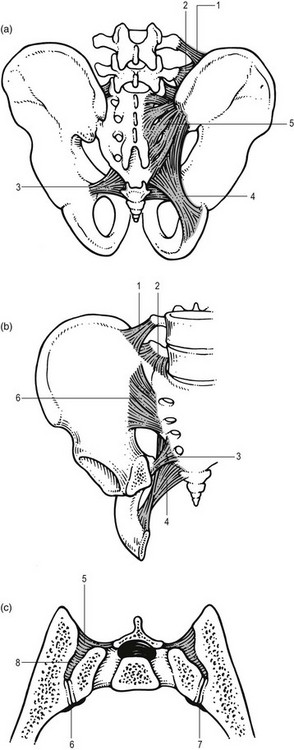
The sacroiliac joint possesses all the characteristics of a true joint: a joint cavity containing synovial fluid,1 adjacent bones having ligamentous connections, cartilaginous surfaces which permit movements and an outer fibrous joint capsule with an inner synovial lining.2–5 The joint most commonly links the posterosuperior part of the medial aspect of the iliac bones with the first, second and the upper part of the third segment of the sacrum (Fig. 1). A transverse section shows that the joint is situated rather anteriorly (Fig. 2). The clinical consequence of this is that it is not possible to elicit tenderness by digital pressure at the joint. The sacrum can be regarded as a wedge that fits vertically between the two iliac bones. The sacrum also fits between these bones in the transversal plane.6 The dorsal width of the sacrum exceeds the ventral width only in the middle portion of the joint (see Fig. 4c). At the lower and upper parts, the wedge shape is quite reversed (see Fig. 2). Several investigators, however, have demonstrated a high degree of variability in the plane of sacroiliac joints, in both the vertical and transverse directions.1,7,8 The articular surfaces are ear- or C-shaped and exhibit irregular ridges and depressions that fit into each other.9,10 The anatomical configuration, together with strong ligaments, make the joint very stable. These features are more pronounced in men than in women, suggesting the likelihood of increased mobility in the latter. Some authors also associate this increased mobility with the position of the centre of gravity, which in women lies dorsal to the hip joint and not in line with the axis of support (Fig. 3). This exerts a strong rotational force in the sacroiliac joint.11,12 Cartilage covers the joint surfaces. It is thicker and smoother at the sacral than at the iliac surface.5 Powerful ligaments support the joint and sharply limit movements (Fig. 4). These ligaments can be divided into the massive interosseous sacroiliac ligament, the posterior and anterior ligaments, and three accessory ligaments – the sacrotuberous, sacrospinous and iliolumbar ligaments. The strong posterior sacroiliac ligament consists of several fascicles of different lengths which overlie the interosseus ligament and pass in an oblique direction from the lateral crests of the sacrum to the posterior superior iliac spine and the posterior end of the inner lip of the iliac crest. Those fibres from the third and fourth sacral segments are longer and constitute the long posterior sacroiliac ligaments.13 The sacroiliac joint is surrounded by some of the largest and most powerful muscles of the body, i.e. the erector spinae, psoas, quadratus lumborum, piriformis, abdominal obliques, gluteal and hamstrings. However, there are no muscles designed to act on the sacroiliac joint to produce active, physiological movements. All muscles that cross the joint are designed to act on the hip or the lumbar spine.1,2,14–16 None of the small movements of the sacroiliac joint is produced by active movements of the sacrum. The movements are indirectly imposed by gravity and muscles acting on trunk and lower limbs. Whether these muscles could contribute to active stability of the joint (force closure) is still open to debate. Some authors suggest that the latissimus dorsi and the contralateral gluteus maximus are coupled via the thoracolumbar fascia. The forces of these two synergists cross the sacroiliac joints perpendicularly and it is hypothesised that this could stabilize the joint indirectly.17–20 No authoritative anatomical studies exist today but most authors report a posterior innervation from the lateral branches of the posterior rami L4–S3 and an anterior innervation from the L2–L3 segments.21 The fact that capsule and ligaments contain nociceptors suggests that the sacroiliac joint is a possible source of low back pain and also plays a role in somatic referred pain.22 The wide range of segmental innervation probably accounts for the variable referred pain patterns seen in sacroiliac joint lesions,1,23 although pain is localized most commonly at the buttock and the posterior thigh.
Applied anatomy of the sacroiliac joint

The joint
Joint capsule and ligaments
Muscles
Innervation
Musculoskeletal Key
Fastest Musculoskeletal Insight Engine