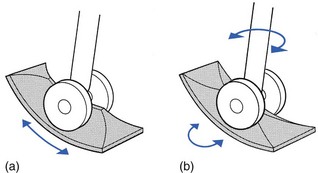
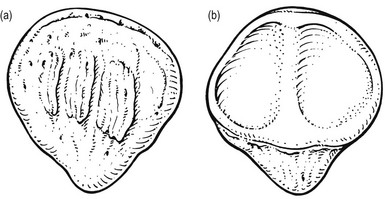
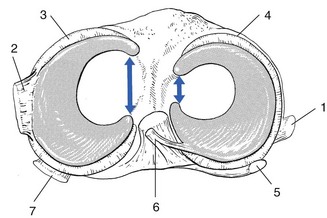
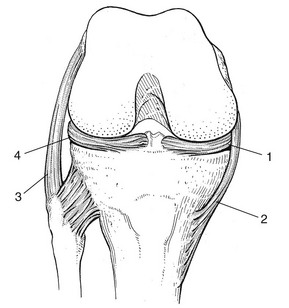
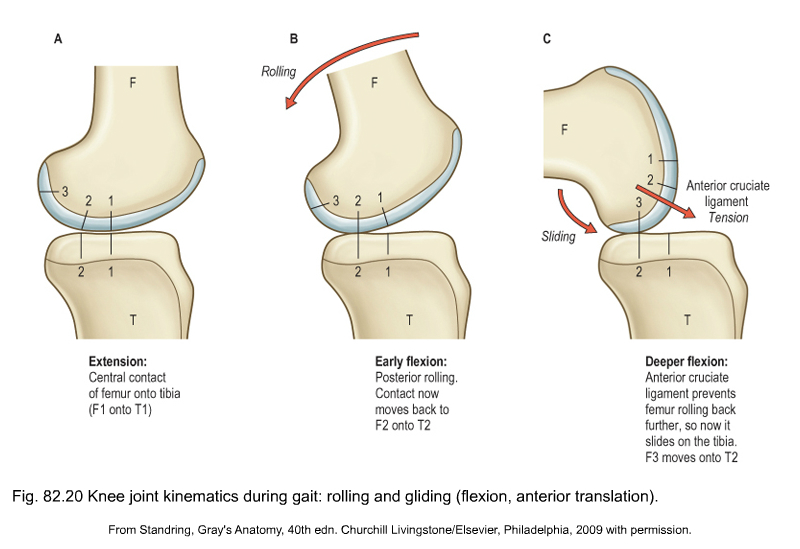
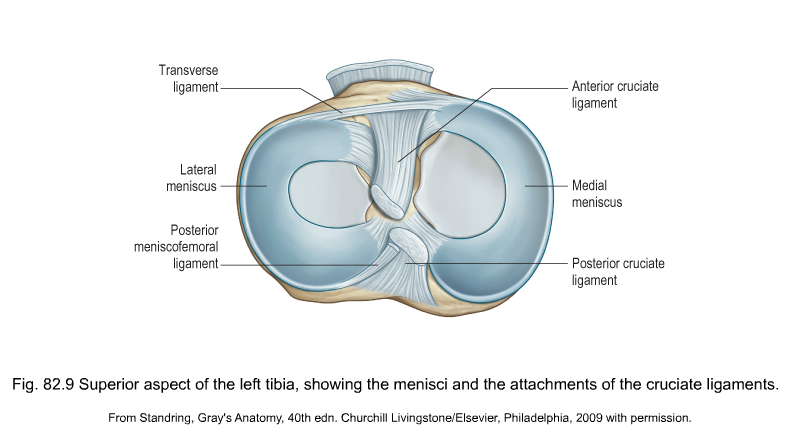
The distal femur can be compared with a double wheel, in which the medial and lateral condyles are the components and the intercondylar notch the junction between them (Fig. 1). The condyles are convex in both planes. The medial condyle extends a little more distally than the lateral. The greater prominence of the lateral femoral condyle prevents the patella from sliding laterally. The anteroposterior elevation between the tibial condyles corresponds to the femoral intercondylar notch. If the surfaces of the tibial condyles are projected anteriorly, they coincide with the articular surface of the patella which corresponds to, and is almost congruent with, the anterior surfaces of the femoral condyles. If the intercondylar eminence of the tibia is projected anteriorly, its plane is continuous with the vertical ridge on the patella just as the intercondylar notch of the femur continues in the central groove of the patellar surface of the femur. This arrangement resembles a twin-wheel rolling on a central rail (Fig. 1a). During flexion and extension, tibia and patella act as one structure in relation to the femur.1 The rounded surfaces of the femoral condyles in relation to the flatter tibial ones might suggest that the former roll during flexion–extension. In fact this is not so. As long ago as 1836 the Weber brothers demonstrated that the femoral condyles roll and slide almost simultaneously, and that these movements are in opposite directions. During flexion, the femoral condyles roll backwards and slide forwards on the tibia, whereas during extension they roll forwards and slide backwards (see Standring, Fig. 82.20). The ratio of rolling to sliding differs with the degree of flexion or extension, which means that during the first 30° of flexion the movement is almost entirely rolling, whereas at nearly full flexion the condyles slip over the tibial plateau without rolling.2 The knee joint is thus primarily a hinge, with the wheel-shaped surfaces of the femoral condyles gliding and rolling in a twin set of concave curved gutters: the tibial and patellar surfaces. However, while this is a satisfactory concept in terms of flexion and extension, in reality the situation is more complex because the knee allows not only gliding and rotation around a horizontal axis but also rotation through a vertical axis, i.e. internal and external rotation of the tibia in relation to the femur. Were the knee to be only as so far described – a hinge joint with a long tibial intercondylar eminence gliding between the two femoral condyles – rotation would be precluded. However, if the anterior and posterior ends are flattened, rotation becomes possible (Fig. 1b). The remaining middle part of the eminence, forming the ‘intercondylar spines’, is then the central pivot about which the movements of axial rotation occur. The patella is a flat, triangular bone, situated on the front of the knee joint (Fig. 2). It is usually regarded as a sesamoid bone, developed in the quadriceps femoris tendon. Its convex anterior surface is covered by an expansion from the tendon of the quadriceps femoris which is continuous below with the superficial fibres of the ligamentum patellae. It is separated from the skin by a bursa (prepatellar bursa). The apex is pointed and gives attachment to the ligamentum patellae. There are two menisci in the space between the femoral and tibial condyles. They are crescent-shaped lamellae, each with an anterior and a posterior horn, and are triangular in cross section. The superior and inferior surfaces are in contact with the femoral and tibial condyles, respectively, and the peripheral surfaces are adherent to the synovial membrane of the capsule. The anterior and posterior horns are anchored to the tibial condyle in the anterior and posterior intercondylar fossae, respectively. The horns of the medial meniscus are further apart than those of the lateral, which makes the former nearly semilunar and the latter almost circular. The menisci correct the lack of congruence between the articular surfaces of tibia and femur, increase the area of contact and improve weight distribution and shock absorption.3–6 They also help to guide and coordinate knee motion, making them very important stabilizers of the knee. Movement between the tibial surface and the menisci is limited by the coronary ligaments connecting the outer meniscal borders with the tibial edge (Fig. 3, see Standring, Fig. 82.9). The coronary ligaments of the medial meniscus are shorter (4–55 mm) and stronger than those of the lateral meniscus (13–20 mm).7 The medial collateral ligament of the knee is attached by its deep fibres to the outer border of the medial meniscus. In contrast, there is no connection between the lateral meniscus and the corresponding collateral ligament (Fig. 4). These anatomical differences between the medial and the lateral meniscus may explain the lesser mobility and the greater vulnerability of the former (see Fig. 3).8 Menisci do not contain pain-sensitive structures and are consequently insensitive to trauma. Their outer third has some blood supply and therefore a slight ability to heal. The inner non-vascularized part receives nutrition through diffusion of synovial fluid.9,10 During flexion of the knee, the body of the meniscus moves posteriorly and during extension it moves anteriorly. In lateral (axial) rotation, the menisci will follow exactly the displacement of the femoral condyles, which means that the lateral meniscus will be pushed forwards on the tibia and the medial meniscus will be pulled backwards (Fig. 5a
Applied anatomy of the knee

Articular surfaces
The patella
The menisci
Movements of the menisci
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


anatomy of the knee

{kind=link}
{kind=link}
