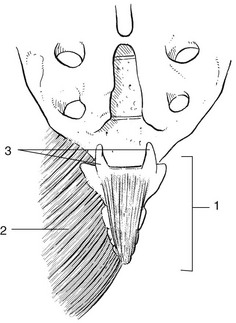
44 The coccyx is formed by fusion of four rudimentary vertebrae. The first coccygeal vertebra has a base for articulation with the apex of the sacrum and two cornua (cornua coccygea) that are usually large enough to articulate with the cornua sacralia. The sacrococcygeal joint is a true joint with a joint capsule and ligaments. Other ligaments covering the posterior aspect of the coccyx are the posterior intercoccygeal ligaments. The gluteus maximus partly inserts at the dorsolateral aspect of the coccyx via its coccygeal fibres (Fig. 44.1). The coccyx and overlying skin are innervated via the dorsal rami of S4 and S5. It is well known that coccygodynia can arise from a lumbar disc lesion, usually as the result of extrasegmental reference.1 Coccygodynia may also arise from irritation of lower pelvic structures (neoplasms of rectum or prostate).2 The history and clinical examination can easily distinguish referred pain from a local disorder. In referred coccygodynia from a disc lesion, pain arises not only during sitting but also during lumbar movements. Coughing is also painful. Physical examination additionally shows pain during lumbar movements, and straight leg raising often increases the discomfort. However, palpation does not assist in diagnosis because local tenderness is to be expected, whichever variety of coccygodynia is present. Tumours or other causes of inflammation affecting the sacrum should be suspected if the pain is not relieved by lying down or if there is nocturnal discomfort. In case of doubt, epidural local anaesthesia can be useful. In ‘idiopathic’ coccygodynia, no particular injury is noted. It has been suggested that certain anatomical variations of the coccyx predispose to repeated microtraumas, which then cause chronic irritation. A coccyx with a sharp forward angle seems to be more prone to painful stretching.3
Anatomy and disorders of the coccyx

Anatomy of the coccyx
Disorders of the coccyx
Referred coccygodynia
Local coccygodynia
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Anatomy and disorders of the coccyx