Figs. 11.1
Snowboarding jump (Photo by Jack Antal)
11.3 Skiing Injuries
The mechanics of skiing involve a separate ski attached to each leg with a binding designed to release in the event of high forces. The independent nature of the two skis means that one ski may move in isolation of the other. During a fall, a ski may catch on the snow and act as a lever arm, creating a torque at the knee. While ski bindings are designed to protect against tibial fracture, they are less effective at protecting the soft tissues of the knee. Consequently, about one-third of all ski injuries involve damage to the soft tissues of the knee [8, 24, 25]. The two most common knee injuries in skiers are medial collateral ligament (MCL) sprains, which can usually be treated non-operatively, and complete ruptures of the anterior cruciate ligament (ACL) which often require surgical intervention [8]. ACL tears in particular, due to their debilitating nature and poor long-term prognostics, are of special concern. Three distinct mechanisms have been identified as the primary causes of ACL tears in recreational skiers [26–28]. The first type of injury known as the boot-induced anterior drawer (BAID) mechanism of ACL injury occurs from an off-balance landing from a jump. If the skier lands with his weight back, the tails of the skis will strike the snow first. The reaction force from the snow creates a moment which drives the ski tips downward. This causes the boot to apply a “passive anterior drawer load” to the tibia which can eventually strain the ACL to rupture [8, 27, 29]. A second mechanism of injury is known as “flexion-internal rotation” or “phantom foot.” This occurs when the skier’s weight is centered over the back of their skis, known in skiing terminology as being in the “backseat.” The skier then loses his/her balance and sits backward toward the slope. The inside edge of the tail of a ski catches the snow and produces a sudden internal rotation of the hyperflexed knee, which tears the ACL. The third mechanism for ACL tear is “valgus-external rotation” also known as a “forward twisting fall.” In this mechanism, the medial edge of the anterior portion of the ski engages the snow, and the skier is propelled forward by their downhill momentum, causing the lower leg to be externally rotated and abducted relative to the thigh [8, 26, 27]. The MCL is thought to be the primary ligament injured in this type of fall, but in 20 % of cases, the ACL is also torn [26, 27].
The phantom foot mechanism of ACL injury was long thought to be the most common cause of ACL injury. However, in the mid-1990s, shorter, specially designed carving skis began to replace traditional longer skis. Since then, the forward twisting fall mechanism has overtaken the phantom foot mechanism as the dominant form of ACL injury in skiers [24, 25, 30]. It is possible that the shorter length of these skis, usually up to the skier’s nose or chin instead of above their heads which was common for traditional skis, limits the ability of the tails to catch the snow and internally rotate the leg while the wider nose of carving skis, designed to help initiate a turn, may itself catch the snow and lead to an increase in the valgus-external rotation of the lower leg during a fall. This pattern seems to hold true for elite level skiers as well. In 2009 Bere et al., described three mechanisms of ACL injury observed in World Cup alpine skiers [29]. One of these mechanisms occurred when the skiers landed out of balance with their weight backward from a jump and appeared similar to the BIAD mechanism described in recreational skiers, although the authors suggested there may be multiple loading conditions that could stress the ACL during such a landing in addition to anterior tibial drawer. The other two mechanisms, the “slip-catch” mechanism and “dynamic snowplow,” occurred when an out-of-balance skier attempted to reestablish snow contact with a ski and the inside edge of their ski abruptly caught the snow surface, forcing the knee into internal rotation and/or valgus relative to the lower leg [29]. Although the conditions leading up the injury are different, the forces applied to the leg seem to be similar to the forward twisting fall seen primarily in recreational skiers in that the inside edge of their carving skis caused forced internal rotation and valgus of the knee, injuring the ACL. Note that while the forward twisting fall mechanism is also known as the “valgus-external rotation,” it is the ski which is being externally rotating while the knee is driven into internal rotation in response.
Knee injuries and especially ACL injuries are several times more common in women than in men [8, 21, 25, 30], possibly due to relative quadriceps weakness in women, lower intercondylar notch dimensions, increased joint laxity, or hormonal differences [8]. In a study of knee injuries of skiers using carving skis, Reudl et al. noted that the bindings did not release in 82 % of falls that resulted in ACL tears in women, while they released in 64 % of similar falls in men [24]. Currently, binding release settings are based on height, weight, foot size, and skier ability, but not gender [31]. It has been suggested that reducing the binding release values by 15 % in female skiers could reduce knee injuries [25].
Another injury unique to skiers compared to snowboarders is a tear of the ulnar collateral ligament (UCL) of the first metacarpophalangeal (MCP) joint [5, 11, 14, 32, 33]. This often occurs when a skier lands on an outstretched hand while holding a ski pole, which causes forced abduction of the thumb and thus ligament damage. This injury is historically so common in skiers that it is also known as “skier’s thumb.” Depending on the severity of the injury, treatment can range from immobilization and eventually gentle physical therapy to, in the case of avulsion, surgical management [32].
Due to the potential high velocities in skiing, it is unsurprising that various fractures occur, most often to the tibia, though these are much less common than knee soft tissue injuries [11, 12, 14]. A substantial number of head, neck, and spine injuries also occur [11, 12, 14, 34], with head injuries being most common among children [12, 34]. This underlies the importance of helmet use, which will be discussed later in this chapter.
11.4 Snowboarding Injuries
The unique mechanics of snowboarding compared to skiing lead to a different injury pattern than seen in skiers. By far the most common injury seen in snowboarders is a wrist sprain or fracture [4, 9–12, 14]. These make up anywhere from 22 to 37.8 % of all snowboarding injuries [4, 9, 11]. Since snowboarders generally do not carry poles, when they fall they often attempt to catch themselves with an open hand, which puts them at risk for injuring their wrist. The shoulder joint is also a common upper extremity injury in snowboarders, especially in experienced riders [9].
Lower extremity injuries are less common in snowboarders than skiers. When they do occur, the leading leg is injured much more frequently than the trailing leg [10]. The mechanism behind this phenomenon is unknown and requires further investigation [10]. Ankle injuries are slightly more common in snowboarders than in skiers, including both ankle sprains and fractures [9, 10, 15, 16]. One particular ankle injury unique to snowboarding is a fracture to the lateral process of the talus, also known as “snowboarder’s ankle.” The proposed mechanism from this injury is a combination of compression and forced inversion or dorsiflexion which may occur when landing from a jump [4, 35]. This injury is important to note because it is frequently missed on plain radiographs and misdiagnosed as a severe ankle sprain [4, 11]. However, conservative management of this type of injury, such as that which would likely occur with an ankle sprain misdiagnosis, can lead to significant disability and osteoarthritis if anatomic alignment is not appropriately maintained [4, 35]. Thus, other imaging techniques such as computed tomography or magnetic resonance imaging are recommended if a snowboarder presents to a clinic with an injured ankle after falling from a jump.
Knee ligament tears are much less common in snowboarding than skiing, most likely due to the fact that the nonreleasable binding system in snowboarders also prevents valgus stress from being applied on one leg, as is seen in the forward twisting fall mechanism of ACL tears common in skiers [14]. ACL tears predominantly occur in expert snowboarders during an improper landing from a large jump, called a flat landing. Normally skiers and riders attempting large jumps in a terrain park aim for the sloped transition of the jump, but when a rider misses the transition, either by jumping too far or not far enough, they land on a flat surface with all the force directed vertically through the leg. During such a landing, the flexion moment on the legs would be resisted by quadriceps. This high level of activation of the quadriceps and low activation of the hamstrings could, in combination with a slightly flexed leg, eccentrically load the knee and strain the ACL to rupture [36]. Studies have reported that another time ACL tears sometimes occur is when only one foot is attached to the snowboard [11]. Snowboarders typically ride with one foot attached to the snowboard when loading and unloading from chairlifts and also when traversing a long, flat area. Falls during these times would allow the snowboard to act as a lever arm in a similar manner to skis and have the potential to injure the ACL.
Snowboarders tend to be at a higher risk of spine injuries and head injuries than skiers [14, 17, 37]. This is mostly likely due to the mechanics of snowboarding which allow for falling backward, thus causing spinal and potentially head trauma. These effects seem to be especially pronounced in beginners [17, 37].
11.5 Skill-Specific Differences
The injury patterns in skiers and snowboarders tend to vary greatly depending on the skill of the participant. Beginners in both sports are responsible for the most injuries though this trend is more pronounced in snowboarding where beginners make up 30–60 % of snowboarding injuries but only 18–34 % of skiing injuries [4, 5, 19, 22, 38]. However, some studies suggest that the injuries sustained by experts in both sports may be more severe [39], which makes sense given the higher travel speeds and more advanced terrain utilized by experts. Expert skiers tend to have greater rates of head, trunk, and upper extremity injuries than beginners. Expert snowboarders tend to have lower rates of upper extremity injuries, especially wrist injuries and head injures [19, 39]. When expert snowboarders experience head and neck injuries, they tend to be less severe, while upper extremity injuries tend to be more severe [39]. Expert snowboarders also suffer a disproportionate number of ACL injuries compared to beginners [10]. As noted above, the predominant mechanism for ACL injuries in snowboarders is jumping related, an activity far more likely to be attempted by experts.
11.6 Risk Factors
Skiing and snowboarding are both high-velocity sports and contain inherent risks. However, there are many factors, both internal and external, that can increase the level of risk (Fig. 11.2).
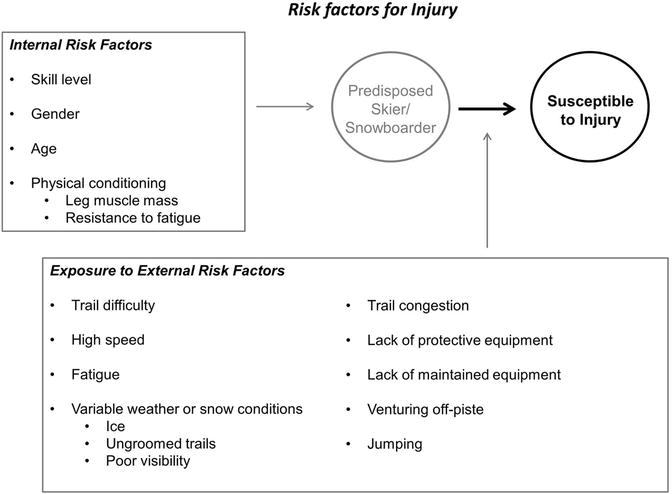
Fig. 11.2
Internal and external risk factors present in skiing and snowboarding
A common factor in injury is skiing or snowboarding past one’s ability level. Attempting a trail above one’s abilities is likely to increase the potential for a fall. Skiing on a run that is too challenging also could have the effect of causing the skier or snowboarder to increase their speed more rapidly than is comfortable and cause them to lose control. Hasler et al. identified “low readiness for speed” as a common cause of injury in snowboarders [40]. Such a situation could arise on a slope that is too steep or too icy for a beginner or intermediate rider or skier.
Skiing and snowboarding are physically demanding sports that require careful focus, awareness, and good form to perform safely, and thus, it is unsurprising that fatigue could increase the risk of injury. Studies show that the majority of ski injuries occur in the afternoon, when skiers and snowboarders are more fatigued [14]. This trend is even present in professional alpine skiers, as most injuries occur during the last fourth of the race [13]. Fatigue has also been shown to have a negative effect on balance [13, 41, 42]. Finally fatigue may cause reaction time to decrease, which could lessen the ability to absorb an impact from an irregularity in the trail or to navigate an obstacle.
High traveling speed has been reported by several sources to be a risk factor for injury [13, 43, 44]. While one source did not report any increase in injury rates in World Cup downhill skiing events with increased travel velocities, the authors suggested that speed could have major impacts on the injury risk in general, which would reduce the ability to anticipate rough terrain and turns, especially when traveling off-piste [40]. Between variable snow conditions, unmarked obstacles, and unpredictable other slope users, a skier and snowboarder must remain in control and able to adapt to their surroundings. However, traveling at a high speed, especially beyond their ability level, reduces the amount of time possible to adjust to these changing conditions. Speed also increases the force of any impact, whether during a fall or with another slope user.
As mentioned above, skiing and snowboarding take place outdoors and while resorts may have some control over snow conditions, for example, creating a more consistent surface by grooming a trail, conditions can change rapidly due to changing temperatures, precipitation, or ski traffic. Soft snow can rapidly turn into an irregular, bumpy surface which can be challenging to navigate especially for beginners. The risk of sustaining a concussion has also been reported to be 2.5 times greater on ungroomed or rough snow compared with soft snow [17]. Skier traffic can scrape off snow and expose ice. Icy conditions have been identified as risk factors in injury [40, 45]. Ice can make it difficult to turn in order to control speed and direction and can also harden the snow, creating a less forgiving surface in the event of a fall. Poor weather and visibility have also been suggested to play a role in the risk of injury. This can be explained by the fact that poor visibility would limit the skier or snowboarder’s ability to navigate around obstacles or prepare for snow irregularity [40, 45].
Finally, the choice of equipment can alter the risk of injury. Using unfamiliar equipment, as is common with beginners using rentals, may prevent a skier or snowboarder from performing optimally. Older equipment may not have effective safety features and, if not maintained, may also perform worse on hard and icy conditions. Specific to skiing, bindings which are not properly adjusted for the skiers’ weight and ability level could either not release early enough during a fall, which could create a torque on the knee with the potential to create injury, or release too soon during normal skiing, causing a fall on their own [20, 46].
11.7 Injury Prevention
Due to the high medical costs incurred by skiing and snowboarding injury, it is important to investigate how we can reduce the number and severity of these injuries. Most studies that have examined strategies to reduce the number of injuries have focused on equipment or behavioral approaches [33].
Head injuries are an important area of concern. While they account for between 3 and 15 % of all injuries, they make up 50–88 % of all skiing and snowboarding fatalities [17]. Helmets are a common-sense protective measure, the effects of which have been investigated in multiple studies. Helmets may reduce the risk of head injuries by 15–60 % [34, 47]. One criticism of helmets is that they might add additional weight to the head and thereby increase the risk of neck injury, a concern especially for children where their head already constitutes a large percentage of their weight. While one study suggested a possible slight increase in risk for neck injury [47], other studies have found no increase in neck injuries in adults [34, 48, 49] or children under 13 [50]. Another concern raised about helmets is the possibility of risk compensation, in which a skier or snowboarder will ride more recklessly due to the added sense of protection imparted by the helmet. However, studies have shown that wearing a helmet does not increase the risk of non-head-related injuries, and thus, no evidence exists for risk compensation [47, 51, 52]. Based on these results, we universally recommend that skiers and snowboarders wear helmets. This is an area where ski resorts can focus their efforts to reduce injuries, such as by requiring children under a certain age to use a helmet. Many provinces in Austria have established mandatory helmet laws for children and adolescents under the age of 16. Interestingly, Ruedl et al. reported that provinces with legislation were shown to increase their helmet use by a smaller percentage than provinces without legislation. Thus, they concluded that mandatory laws may increase rates of helmet use in provinces where use is already low, but public education may be as effective as mandatory laws [53]. Helmet use was also observed to be lower in adolescents 16 and older in provinces where helmets were not mandatory [53]. A more recent study of Austrian children reported that helmet laws in combination with an educational campaign increased self-reported helmet use to 99 % for children under 16, which then decreased to 91 % for children 16 and older. Interestingly enough, the rate of helmet use for adolescents over 16 was lower in provinces where helmet use laws were in effect than in provinces where they were not, suggesting that making helmets mandatory decreases compliance in children above the restricted age, where they may view the option to not wear helmets as a new freedom [54]. Several public education campaigns to promote helmet use are already in existence, for example, the “Lids on Kids” campaign promoted by the National Ski Areas Association (NSAA) in the United States, which encourages the use of helmets in children. Due in part to these campaigns, helmet use in skiing and snowboarding is higher than it has ever been in the United States, with 70 % of all skiers and snowboarders, 80 % of skiers and snowboarders under the age of 18, and nearly 90 % of children ages 9 and under wearing them [55]. Note that these rates of helmet use are much lower than in Austria, but also note that the overall helmet use rates in Austria were higher than the United States in all provinces, regardless of mandatory helmet laws, suggesting a cultural difference in attitudes toward helmet use between the two countries. Whether mandatory helmet laws are the best method for increasing helmet use is a topic for debate.
Since the most common injuries in snowboarders are wrist sprains and fractures, wrist guards have been investigated as a potential tool to reduce the rate of these injuries. Wrist guards have been shown to reduce the risk of wrist and forearm injuries between 52 and 82 % [56–58]. Despite this, very few snowboarders choose to wear them. While wrist guards may decrease the risk of wrist injuries, some studies have found an increase in shoulder and elbow injuries when wrist guards are used [56]. Landing on the forearm with an extended elbow while wearing a wrist guard may make the arm act as a lever with the fulcrum at the point of impact and transfer a torque to the shoulder joint. Furthermore, the studies that have looked at the use of wrist guards have generally ignored the many different designs of wrist guards, and thus, not enough study has been done to say which, if any wrist guards provide the most protection while reducing the risk of shoulder injury. At this time there is not enough evidence to universally recommend the use of wrist guards for experienced snowboarders where the risk of wrist injuries is already relatively low, and more research should be done to determine if they should be recommended for beginners, who are at the highest risk of wrist injury.
As noted above, properly maintained equipment, especially properly adjusted ski bindings, can help reduce the risk of injury [20, 46]. Properly adjusted bindings will release when the forces generated by a fall are sufficient, and bindings that are too tight will not release in the event of a fall and can potentially generate enough torque to injure a skiers’ knee. Regularly sharpened skis can more easily maintain purchase and help skiers maintain control on hard and icy conditions, which have been noted as a risk factor in injury [40, 45].
Another substantial cause of injury is overestimating one’s ability level or not properly assessing the snow conditions. Fortunately, virtually all ski resorts in North America and most throughout the world grade and mark their trails with a difficulty rating from beginner to advanced terrain. While this is important, the categories can be broad and the difference, for example, between a beginner and intermediate trail is relative to the other trails on the mountain. Furthermore, conditions can easily change what would normally be an easy run into a hazardous one. Many mountains post daily condition reports which state whether a trail is groomed, ungroomed, has fresh powder, or other important slope information which can give a skier or rider an idea of the conditions prior to attempting a trail. Another way that this could be addressed is to include training about assessing conditions and also understanding one’s limits when taking lessons. Counterintuitively, taking ski or snowboard lessons has not been shown to decrease the risk of injury [38, 46]. This may be because lessons tend to be focused on the rapid acquisition of skill as opposed to safety education and that individuals who take lessons often take them sporadically which may not be enough to instill safe habits. Ski lessons could potentially improve the rates of injury by placing an emphasis on acquiring this knowledge as well as learning physical techniques.
Other training methods to reduce injury may be of interest. Ettlinger et al. demonstrated that injuries to the ACL could be reduced by 62 % using a training session in which participants were involved in interactive video and physical instruction to identify movement patterns which could contribute to the phantom foot mechanism of ACL injury [59]. Using instructional ski videos alone, Jørgensen et al. were able to show a 30 % reduction in ski injuries compared to those who had not been shown the videos [60]. Since the publication of these articles, the sport of skiing has evolved substantially, especially with the advent of carving skis in the mid-1990s which altered the pattern of ACL injuries such that the forward twisting fall mechanism of ACL tear is now the more dominant. However, these two approaches could be adapted using modern ski equipment, with focus on the forward twisting fall mechanism of ACL tear. If these methods prove to be effective, instructional videos could be spread using the internet and social media services to reach the largest number of skiers.
Finally, one area that could be addressed is musculoskeletal conditioning regimens and neuromuscular training specific to skiing and snowboarding. A similar strategy has been implemented in soccer using a program known as the “FIFA 11+” which includes cardiovascular conditioning, core and leg strength, and balance and agility, can be completed in 20 min as a warm-up prior to a match or training, and has been shown to reduce training injuries by 37 %, match injuries by 29 %, and severe injuries by 50 % [61]. A skiing-specific training regimen was suggested by Morrissey in 1987 which included stretches, resistance, and cardiovascular training specific to the activities involved in skiing [62]. While parts of this training could be applied to modern skiing, with the advent of shaped skis, the mechanics and musculature involved in skiing are likely very different. Furthermore, to our knowledge, nothing similar has been proposed for the sport of snowboarding, which utilizes completely different mechanics than skiing. Such neuromuscular training could be useful for preventing skiing and snowboarding injuries. However, there currently exists minimal information in the literature that suggests conditioning or strength training routines or even individual exercises that could be used to prevent injury in skiing or snowboarding [33]. Further research must be conducted to identify exercises which could be incorporated into neuromuscular training programs specific for skiing and snowboarding and would ideally include activities that can be performed easily in ski and snowboard boots prior to taking the first run of the day.
11.7.1 Extreme Terrain
11.7.1.1 Off-Piste Terrain
The vast majority of skiing and snowboarding accidents take place on maintained slopes run by ski resorts (“on-piste”). However, it is common for advanced and expert skiers and snowboarders to venture off the relative safety of these maintained slopes into unmaintained trails in search of fresher snow, more challenging terrain, and fewer crowds. This is known as going “off-piste.” While most of the normal risks of alpine skiing and snowboarding are still present when venturing off trail, additional risks present themselves, including natural hazards such as the risk of avalanche, cliffs, rocks, and other unmarked obstacles, as well as additional risks encountered when traveling in isolated regions in the mountains such as frostbite, hypothermia, dehydration, fatigue, acute mountain sickness, and sunburn.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


