Adamantinoma of Long Bones
Adamantinoma of long bones is a peculiar neoplasm that, on the basis of radiographic and pathologic features, arises within the osseous substance. The origin of the epithelial islands in this tumor is unknown. Immunohistochemical and electron microscopy studies have confirmed the epithelial nature of these islands. It has been postulated that traumatic implantation of epithelium is the cause of these tumors because almost all reported adamantinomas have occurred in bone near the cutaneous surface. Others have considered congenital rests of epithelium as the source of the tumors, and still others have stated that the so-called adamantinoma of long bones is not epithelial at all but represents an unusual manifestation of sarcoma, either synovial sarcoma or angiosarcoma.
In 1957, Changus and coauthors proposed that the tumor had an angioblastic origin. Many of the histologic features would favor this concept. Many tumors have a vascular appearance, with the cells that line spaces apparently continuous with obvious epithelial cells. However, endothelial markers have not been positive in the neoplastic cells and, as mentioned elsewhere, epithelial markers have.
Despite this controversy, the fact remains that adamantinomas of long bones comprise a small group of distinctive tumors that present as primary lesions of bone. It is possible that several histogenetically different tumors can produce the features of adamantinoma. None of the proposed theories of origin explains its peculiar predilection for the tibia.
The name adamantinoma was given to this tumor because of its histologic resemblance to the more common adamantinoma (ameloblastoma) of the jawbones. These odontogenic tumors of the jaws and the histologically related tumors that arise from Rathke pouch are obviously not related and are excluded from the discussion that follows.
INCIDENCE
There are 44 examples of adamantinoma of long bones in the Mayo Clinic files (Fig. 24.1). This represents 0.56% of the malignant primary tumors of bone. In 1986, Moon and Mori collected 180 cases from the literature and added 15 of their own.
SEX
In this series, there was a slight male predominance, similar to other reports in the literature.
AGE
The majority of patients with adamantinoma are adolescents and young adults. Approximately 72% of all patients in this series were in the second and third decades of life. Only two patients were in the first decade of life; both were 7 years old: one girl and one boy with lesions of the mid tibia. The oldest patient was a 79-year-old man, who also had a lesion of the mid tibia.
LOCALIZATION
Of all reported adamantinomas of long bones, 90% have involved the tibia, although examples have been found in all the long tubular bones. Some cases of adamantinoma have also been reported in short tubular bones, but the diagnoses in these cases have to be considered suspect. Of the 43 lesions (in 40 patients) in the Mayo Clinic series, 34 involved the tibia: 29 involved the mid tibia, and 5 involved the distal metaphysis. Four patients had involvement of the fibula: two in the
mid portion and two in the lower portion. One of the patients with involvement of the fibula was treated in 1951 and returned 17 years later with a lesion of the tibia. One patient had synchronous involvement of the tibia and fibula. The other two had involvement only of the fibula. In the series reported by Keeney and coauthors, 70 of the 85 patients had a tumor in the tibia. Eleven of these patients also had involvement of the ipsilateral fibula. The other cases were distributed as follows: two in the distal ulna, one in the mid radius, and two in the femur (one in the mid portion and one in the lower portion).
mid portion and two in the lower portion. One of the patients with involvement of the fibula was treated in 1951 and returned 17 years later with a lesion of the tibia. One patient had synchronous involvement of the tibia and fibula. The other two had involvement only of the fibula. In the series reported by Keeney and coauthors, 70 of the 85 patients had a tumor in the tibia. Eleven of these patients also had involvement of the ipsilateral fibula. The other cases were distributed as follows: two in the distal ulna, one in the mid radius, and two in the femur (one in the mid portion and one in the lower portion).
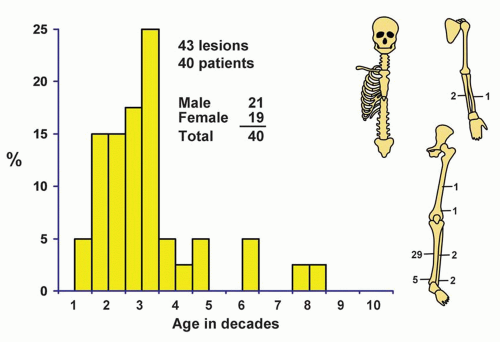 Figure 24.1. Distribution of adamantinomas according to age and sex of the patient and site of the lesion. |
SYMPTOMS
The prolonged clinical course of many of the patients with this tumor indicates its generally slow growth. Pain is the most common initial symptom, although local tumefaction is the first complaint of a few patients. The duration of symptoms before diagnosis has varied from a few months to 50 years. In the series reported by Keeney and coauthors, approximately one-third of the patients had symptoms for more than 5 years. Pathologic fracture is uncommon.
PHYSICAL FINDINGS
A mass, which may be painful, is the only physical finding of consequence.
RADIOGRAPHIC FEATURES
The most common, or typical, appearance is that of multiple, sharply circumscribed, lucent defects of different sizes with sclerotic bone interspersed between the zones and extending above and below the lucencies. Some of the lucent zones are small, entirely cortical, and similar to those seen in osteofibrous dysplasia. Rarely, the rarefied area is elongated and located predominantly within the medullary cavity, with a zone of irregular sclerosis at its margins. Typically, one of the lytic areas, usually in the mid shaft of the bone, is larger and more destructive appearing. When both the tibia and the fibula are involved, the appearance is consistently as described. The multiple lucent zones may represent multifocal involvement initially, but because the intervening bone is abnormally sclerotic, these zones probably represent one lesion (Figs. 24.2, 24.3, 24.4 and 24.5).
Rare lesions of various bones have presented as large, multilobulated lucent areas with expansion and thinning of the cortex. The most frequent differential problem is osteofibrous dysplasia.
GROSS PATHOLOGIC FEATURES
Ordinarily, adamantinomas are clearly delimited peripherally, as indicated on radiographs. The contours of these tumors are often lobulated. Most of the tumors are gray or white, and they vary in consistency from
firm and fibrous to soft and brainlike (Fig. 24.6). They may contain spicules of bone and calcareous material. Cystic cavities, which may contain blood or clear fluid, are sometimes encountered. Some of the tumors erode through the overlying cortex, but this is unusual in patients who have not undergone a prior surgical procedure. As mentioned above, a few adamantinomas have been distinctly eccentric, not involving the medulla but confined to the cortex. An occasional adamantinoma has been described in the soft tissues adjacent to the tibia.
firm and fibrous to soft and brainlike (Fig. 24.6). They may contain spicules of bone and calcareous material. Cystic cavities, which may contain blood or clear fluid, are sometimes encountered. Some of the tumors erode through the overlying cortex, but this is unusual in patients who have not undergone a prior surgical procedure. As mentioned above, a few adamantinomas have been distinctly eccentric, not involving the medulla but confined to the cortex. An occasional adamantinoma has been described in the soft tissues adjacent to the tibia.
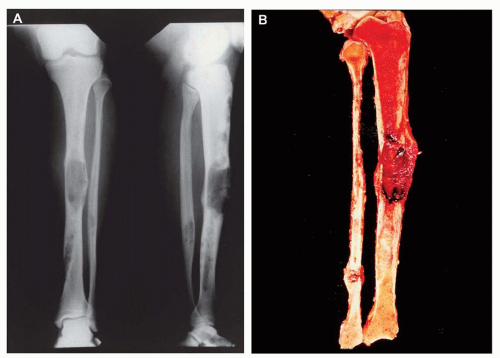 Figure 24.2. Adamantinoma involving the tibia and fibula in a 19-year-old woman. A: Extensive involvement of the cortex of the tibia includes a large destructive area in the mid portion. This appearance is quite typical. The lower fibular shaft is also involved. B: Corresponding gross specimen. The cortical involvement is much more extensive than the obvious large destructive areas in the mid portion of the tibia. |
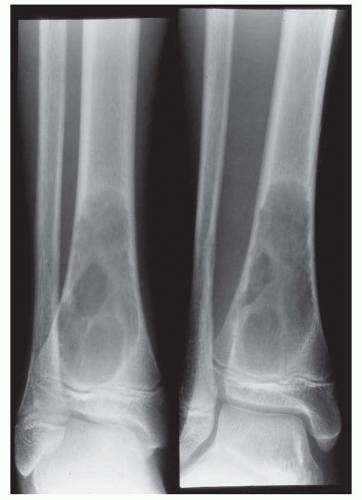 Figure 24.3. The radiographic appearance is sometimes atypical, as in this distal tibial lesion in a 14-year-old boy. The appearance is nonspecific. |
HISTOPATHOLOGIC FEATURES
Various histologic patterns have been described, but all of them have an epithelial quality. The typical histologic appearance is that of small epithelial islands in a fibrous stroma (Figs. 24.7, 24.8, 24.9 and 24.10




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
