Acetabulum
EPIDEMIOLOGY
The incidence of acetabular fractures is 3 per 100,000 population per year.
Neurologic injuries occur in up to 30% of cases and are usually partial injuries to the sciatic nerve, with the peroneal division more commonly injured than the tibial division.
ANATOMY
From the lateral aspect of the pelvis, the innominate osseous structural support of the acetabulum may be conceptualized as a two-columned construct (Judet and Letournel) forming an inverted Y (Fig. 26.1).
Anterior column (iliopubic component): This extends from the iliac crest to the symphysis pubis and includes the anterior wall of the acetabulum.
Posterior column (ilioischial component): This extends from the superior gluteal notch to the ischial tuberosity and includes the posterior wall of the acetabulum.
Acetabular dome: This is the superior weight-bearing portion of the acetabulum at the junction of the anterior and posterior columns, including contributions from each.
Corona mortis
A vascular communication between the external iliac or deep inferior epigastric and the obturator may be visualized within the Stoppa or second window of the ilioinguinal approach.
Present in up to 10% to 15% of patients
May extend over the superior pubic ramus; average distance from the symphysis to corona, 6 cm
Ascending branch of medial circumflex
Main blood supply to femoral head
Deep to quadratus femoris
Superior gluteal neurovascular bundle
Emerges from the greater sciatic notch
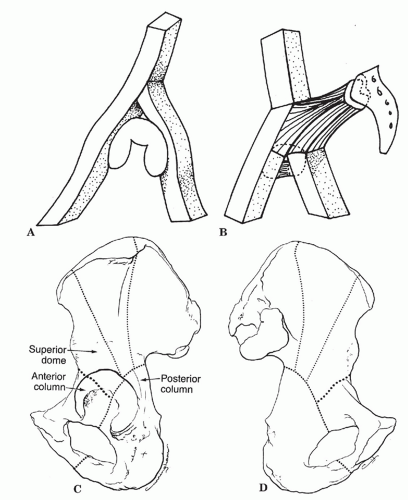 FIGURE 26.1 (A) A diagram of the two columns as an inverted Y supporting the acetabulum. (B) The two columns are linked to the sacral bone by the “sciatic buttress.” (C) Lateral aspect of the hemipelvis and acetabulum. The posterior column is characterized by the dense bone at the greater sciatic notch and follows the dotted line distally through the center of the acetabulum, the obturator foramen, and the inferior pubic ramus. The anterior column extends from the iliac crest to the symphysis pubis and includes the entire anterior wall of the acetabulum. Fractures involving the anterior column commonly exit below the anterior-inferior iliac spine as shown by the heavy dotted line. (D) The hemipelvis from its medial aspect, showing the columns from the quadrilateral plate. The area between the posterior column and the heavy dotted line, representing a fracture through the anterior column, is often considered the superior dome fragment. (From Letournel E, Judet R. Fractures of the Acetabulum. New York: Springer-Verlag; 1964.) |
MECHANISM OF INJURY
Like pelvis fractures, these injuries are mainly caused by high-energy trauma secondary to a motor vehicle, motorcycle accident, or fall from a height.
The fracture pattern depends on the position of the femoral head at the time of injury, the magnitude of force, and the age of the patient.
Direct impact to the greater trochanter with the hip in neutral position can cause a transverse type of acetabular fracture (an abducted hip causes a low transverse fracture, whereas an adducted hip causes a high transverse fracture). An externally rotated and abducted hip causes an anterior column injury. An internally rotated hip causes a posterior column injury.
With indirect trauma (e.g., a “dashboard”-type injury to the flexed knee), as the degree of hip flexion increases, the posterior wall is fractured in an increasingly inferior position. Similarly, as the degree of hip flexion decreases, the superior portion of the posterior wall is more likely to be involved.
CLINICAL EVALUATION
Trauma evaluation is usually necessary, with attention to airway, breathing, circulation, disability, and exposure, depending on the mechanism of injury.
Patient factors such as patient age, degree of trauma, presence of associated injuries, and general medical condition are important because they affect treatment decisions as well as prognosis.
Careful assessment of neurovascular status is necessary because sciatic nerve injury may be present in up to 40% of posterior column disruptions. In rare cases, it may be entrapped within the posterior column fracture. Femoral nerve involvement with anterior column injury is rare, although compromise of the femoral artery by a fractured anterior column has been described.
The presence of associated ipsilateral injuries must be ruled out, with particular attention to the ipsilateral knee in which posterior instability and patellar fractures are common.
Soft tissue injuries (e.g., abrasions, contusions, presence of subcutaneous hemorrhage, Morel lesion) may provide insight into the mechanism of injury.
RADIOGRAPHIC EVALUATION
An anteroposterior (AP) and two Judet views (iliac and obturator oblique views) should be obtained.
AP view: Anatomic landmarks include the iliopectineal line (limit of anterior column), the ilioischial line (limit of posterior column), the anterior wall, the posterior wall, the line depicting the superior weight-bearing surface of the acetabulum, and the teardrop (Fig. 26.2).
Iliac oblique radiograph (45-degree external rotation view): This best demonstrates the posterior column (ilioischial line), the iliac wing, and the anterior wall of the acetabulum (Fig. 26.3). (I.O.W.A. = Iliac Oblique Wall Anterior)
Obturator oblique view (45-degree internal rotation view): This is best for evaluating the anterior column and posterior wall of the acetabulum (Fig. 26.4).
Computed tomography (CT): This provides additional information regarding size and position of column fractures, impacted fractures of the acetabular wall, retained bone fragments in the joint, degree of comminution, and sacroiliac joint disruption. Three-dimensional reconstruction allows for digital subtraction of the femoral head, resulting in full delineation of the acetabular surface.
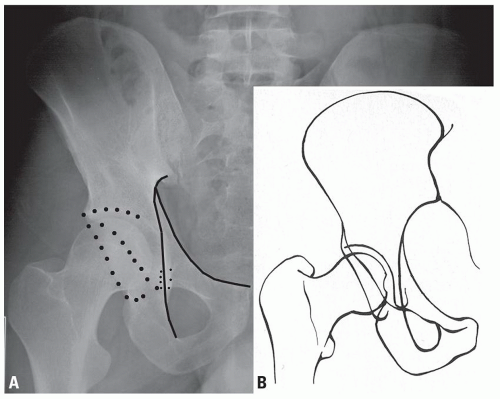 FIGURE 26.2 (A, B) Diagram outlining the major landmarks: the iliopectineal line (anterior column), the ilioischial line (posterior column), the anterior lip of the acetabulum, and the posterior lip of the acetabulum. (From Bucholz RW, Heckman JD, eds. Rockwood and Green’s Fractures in Adults. 5th ed. Baltimore: Lippincott Williams & Wilkins; 2002.) |
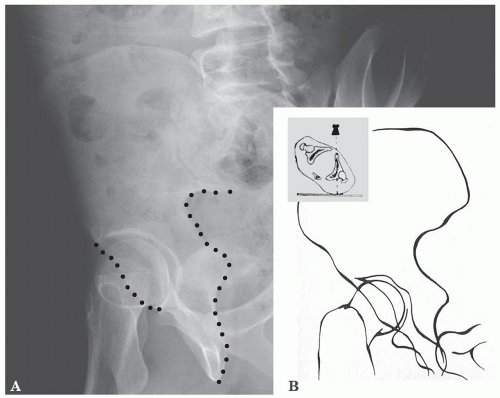 FIGURE 26.3 Iliac oblique view. (A) This view is taken by rotating the patient into 45 degrees of external rotation by elevating the uninjured side on a wedge. (B) Diagram of the anatomic landmarks of the left hemipelvis on the iliac oblique view. This view best demonstrates the posterior column of the acetabulum, outlined by the ilioischial line, the iliac crest, and the anterior lip of the acetabulum. (From Tile M. Fractures of the Pelvis and Acetabulum. 2nd ed. Baltimore: Williams & Wilkins; 1995.) |
CLASSIFICATION
Judet-Letournel
Classification describes the fracture pattern, there are 10 fracture patterns, 5 “elementary” and 5 “associated” (Fig. 26.5).
|
Elementary Fractures
Posterior wall fracture
This involves a separation of posterior articular surface.
Most of the posterior column is undisturbed (ilioischial line is not broken).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








