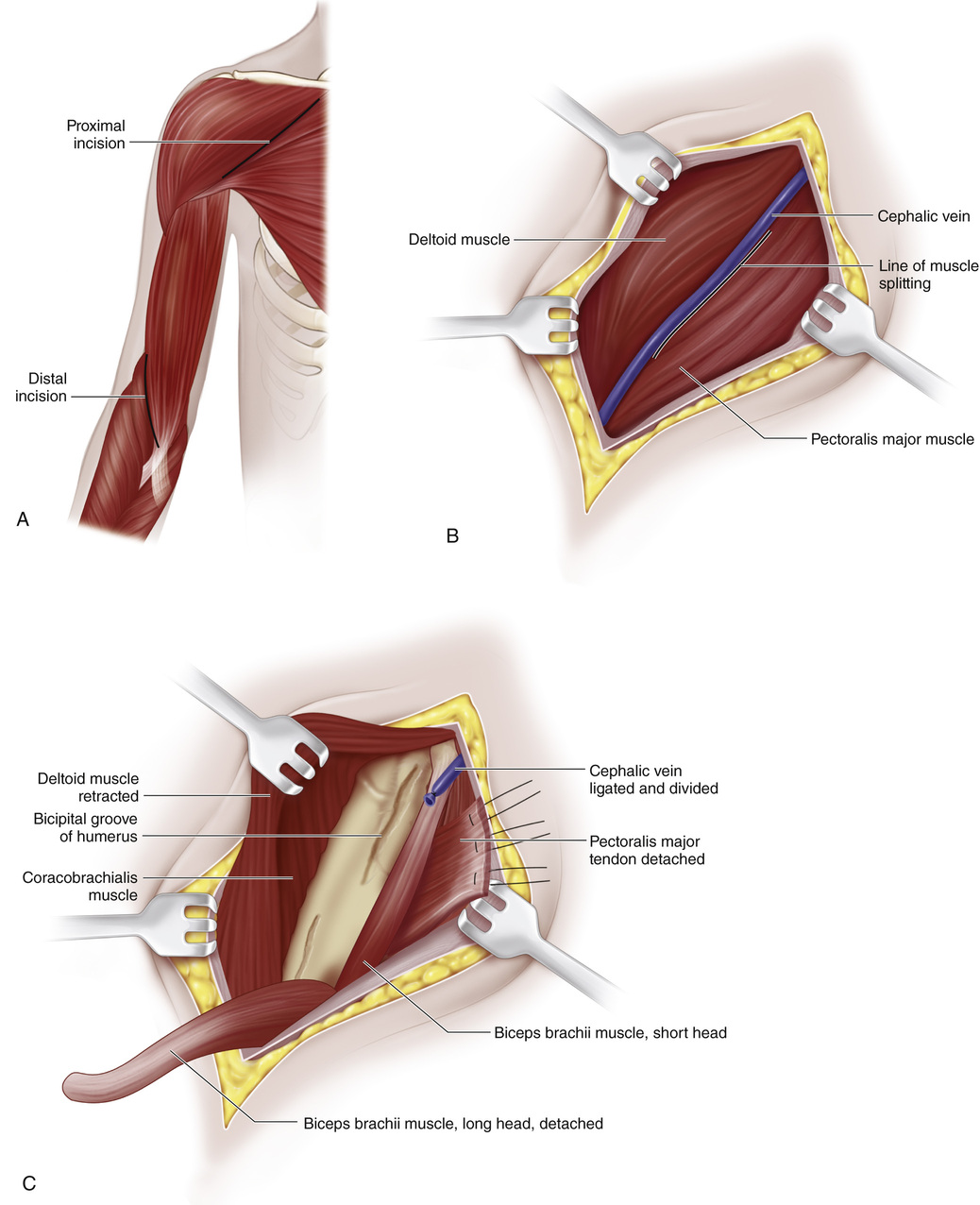
A, The patient is positioned supine with the upper limb supported on a hand table and the shoulder in 45 degrees of abduction and 30 degrees of external rotation. Two incisions are made, the first one following the deltopectoral groove and extending from the clavicle down to the junction of the upper and middle thirds of the arm. The second incision is centered over the anteromedial aspect of the elbow. B, Through the first incision the subcutaneous tissue and deep fascia are divided, and the cephalic vein is ligated if necessary. C, The pectoralis major tendon is identified and divided at its insertion, as close to the bone as possible. By blunt dissection the muscle is mobilized from the chest wall toward the clavicle. The deltoid muscle is then retracted laterally and the tendon of the long head of the biceps is exposed as it runs upward toward the shoulder joint. It is severed at the upper end of the bicipital groove and pulled distally into the wound. D, By blunt and sharp dissection, the muscle belly of the long head of the biceps is mobilized to the lowest third of the arm by freeing it from the short head. The vessels and nerves entering the muscle belly are divided and ligated as necessary. The tendon and muscle of the long head are delivered into the distal second incision and freed down to the tuberosity of the radius. Often, freeing the muscle from adhesions to the overlying fascia requires sharp dissection. After complete mobilization of the long head of the biceps by traction on its proximal end, the operator should be able to flex the elbow. E, The long head of the biceps is pulled into the upper wound. Two slits are made in the tendon of the mobilized pectoralis major through which the tendon of the long head is passed, looped on itself, and brought down again into the distal wound. With the elbow acutely flexed, the proximal end of the tendon is sutured to its own tendon of insertion through a slit in the distal part of the tendon. Silk sutures are also inserted at the level of the tendon of the pectoralis major. The incisions are then closed in routine manner. A plaster-of-Paris–reinforced Velpeau bandage is applied with the elbow acutely flexed.
Pectoralis Major Transfer for Paralysis of the Elbow Flexors
Operative Technique

Related posts:
 23 Hamstring Lengthening
23 Hamstring Lengthening
 29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
 10 Pemberton Osteotomy
10 Pemberton Osteotomy
 33 Triple Arthrodesis
33 Triple Arthrodesis
 38 Exposure of the Spine for Posterior Instrumentation and Fusion
38 Exposure of the Spine for Posterior Instrumentation and Fusion
 42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


