Modified Green Scapuloplasty for Congenital High Scapula (Sprengel Deformity)
First, an osteotomy of the clavicle is performed. The patient is placed in the lateral decubitus position, and the upper half of the chest, the entire neck, the entire upper limb, and the posterior aspect of the neck are fully prepared and draped. It is vital that the level of the contralateral normal scapula be visible during surgery. An alternative method is to place the patient in the supine position and prepare the neck and upper half of the chest, perform the osteotomy of the clavicle, and then turn the patient to the prone position and reprepare and redrape. This author finds it expedient to use the former method.
Operative Technique
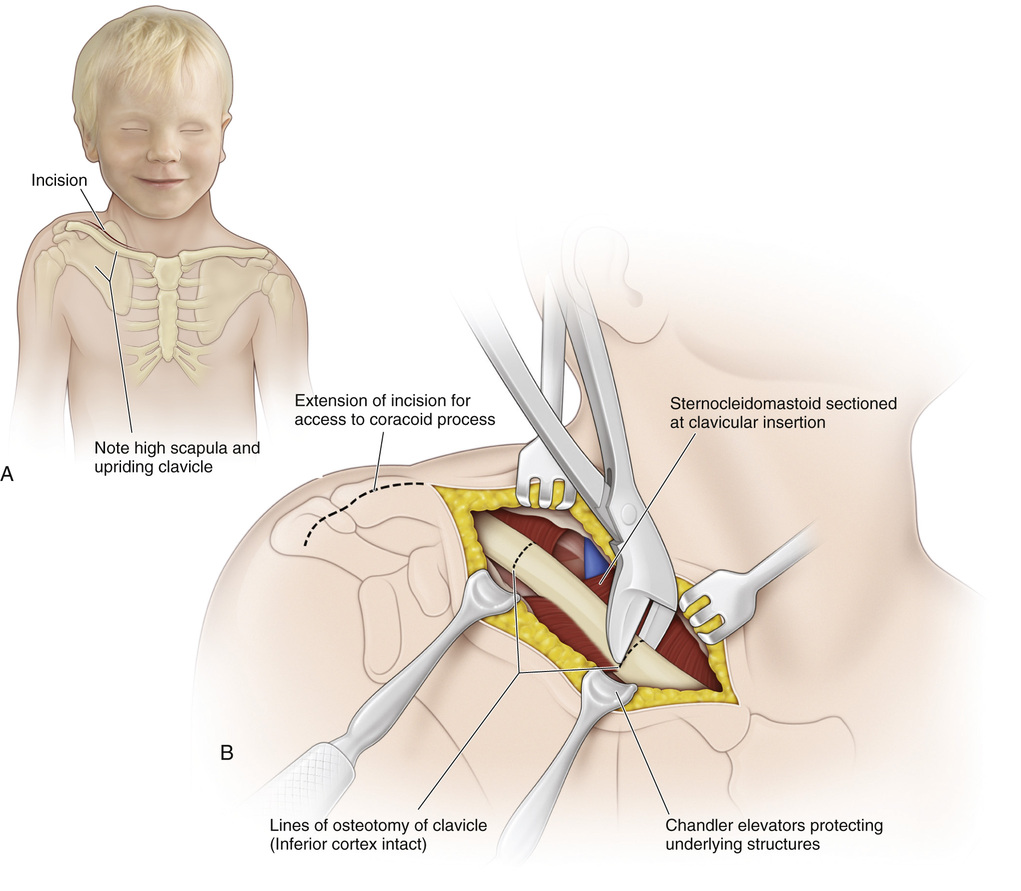
A, A supraclavicular curvilinear incision is made 2 cm above the clavicle in line with the skin creases of the neck and centered over the midportion of the clavicle. It is best to make the skin incision with the neck in slight flexion (not hyperextension). The subcutaneous tissue is divided in line with the skin incision, and the wound is pulled down directly over the clavicle.
B, The deep fascia is incised; any superficial veins are clamped and coagulated. The periosteum of the clavicle is divided longitudinally on its anterior aspect and, with a periosteal elevator, is gently elevated circumferentially around the clavicle. Two smaller Chandler elevators are placed deep to the clavicle to protect the subclavicular vessels and the brachial plexus.
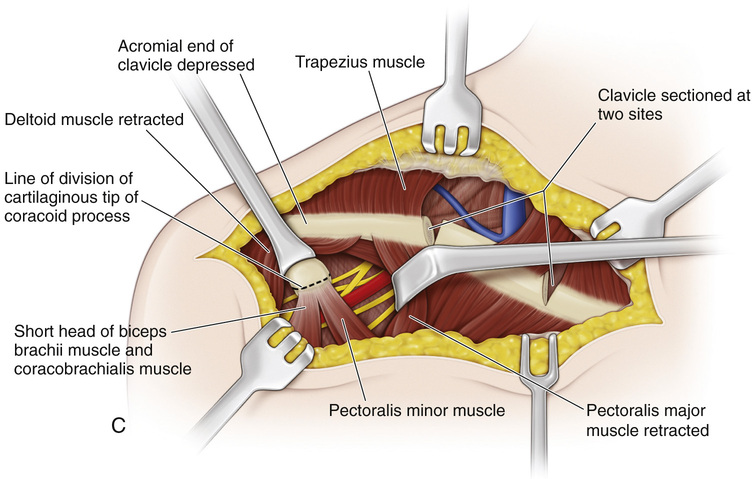
C, With a bone cutter or an oscillating electric saw, the clavicle is sectioned at one or two sites with its posteroinferior cortex left intact (if two sites are used, they should be 3 cm apart). Then by gentle force, a greenstick fracture of the clavicle is produced. The periosteum is closed. The skin is closed with subcuticular running suture. Morcellation of the clavicle is not recommended.
In an older patient the incision may be extended laterally so that the tip of the coracoid process and the origins of the short head of the biceps brachii and the coracobrachialis muscles are exposed. The cartilaginous tip of the coracoid process is sectioned, and then the wound is closed as already described. The purpose of this step in a child older than 10 years is to prevent compression of the neurovascular bundle against the rib.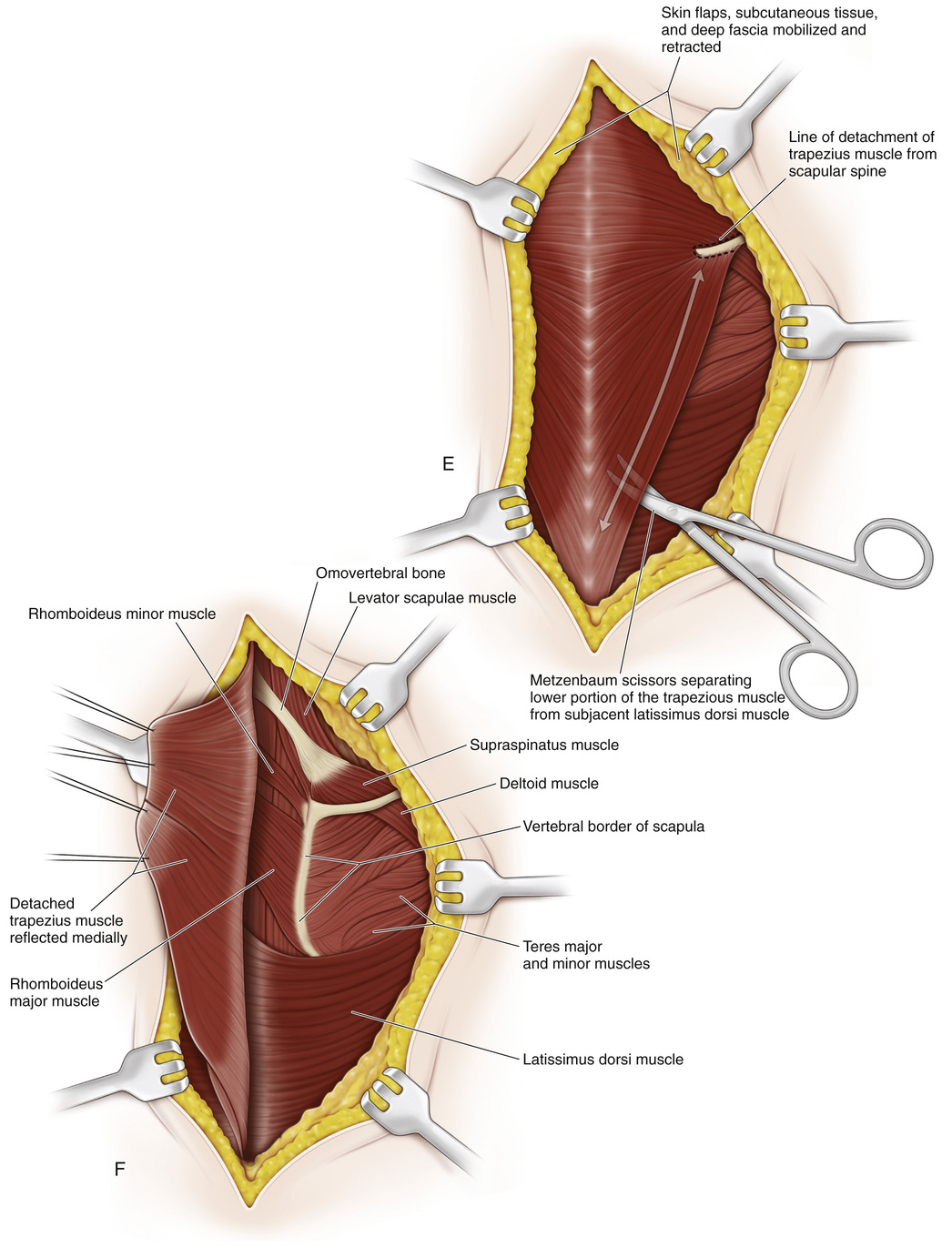
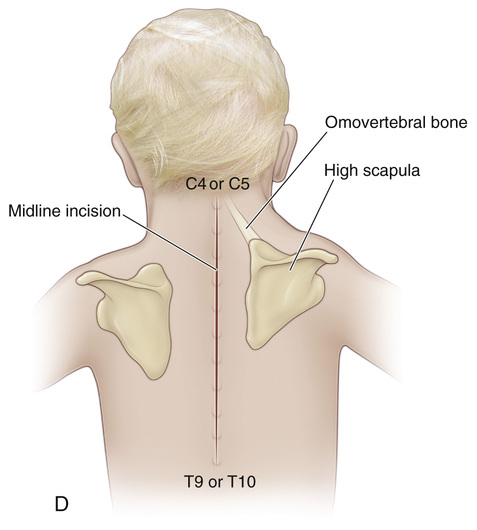
D, The patient is turned to the prone position with the head and neck extending beyond the operating table and supported on a headrest. The chin piece of the headrest should be well padded, and during the procedure the anesthesiologist should frequently check the chin for pressure areas. Anchoring the buttocks to the operating table with 2- or 3-inch-wide adhesive tape will prevent the patient from slipping caudally. Care should be taken to guard the sterility of the operating field. First, the vertebral border, the level of the inferior angle and the spine of the elevated scapula, and those of the opposite normal scapula are palpated and marked with indelible ink. A midline skin incision is made that begins at the spinous process of the fourth cervical vertebra and extends distally to terminate at the spinous process of the tenth dorsal vertebra (C4 to T10).
E, The skin and subcutaneous tissue are divided in line with the skin incision, and a place between the subcutaneous tissue and fascia underlying the trapezius muscle is developed. Dissection is extended laterally to expose the spine of the scapula. Next, the inferior margin of the trapezius muscle, which runs obliquely upward and laterally to the scapular spine, is isolated. Its free lateral border is mobilized and retracted proximally and medially. The insertion of the entire trapezius muscle (superior, middle, and inferior parts) on the scapular spine is sectioned, elevated extraperiosteally, and marked with 2-0 Mersilene suture. Inferiorly, the lower fibers of the trapezius muscle are separated from the subjacent latissimus dorsi muscle with Metzenbaum scissors.
F, The detached trapezius muscle is reflected medially to expose the underlying muscles and scapula. The spinal accessory nerve, which is the motor nerve of the trapezius, should not be injured.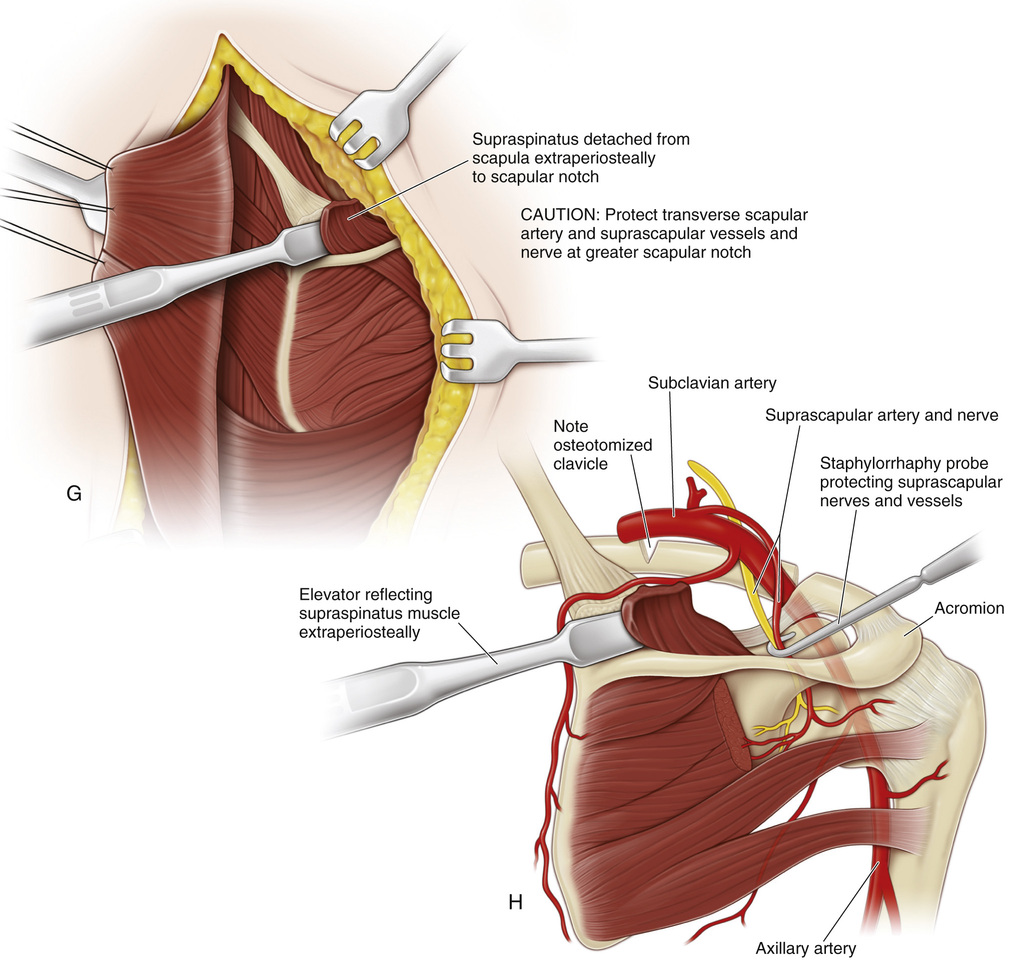
G and H, The supraspinatus muscle is then detached from the scapula extraperiosteally to the greater scapular notch. The transverse scapular artery and suprascapular vessels and nerve must be identified and protected in the lateral portion of the wound as they enter the infraspinatus fossa and pass through the greater scapular notch.
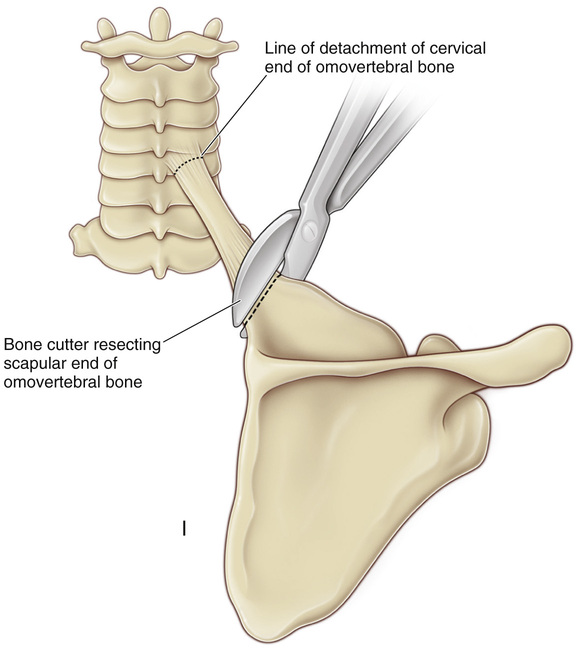
I, The omovertebral bar (bony, cartilaginous, or fibrous) is excised by first sectioning it at the scapular end with a bone cutter and then gently detaching its attachment to the cervical vertebra. At the cervical level it may be attached to the spinous process, lamina, or transverse process of one of the lower cervical vertebrae (fourth to seventh).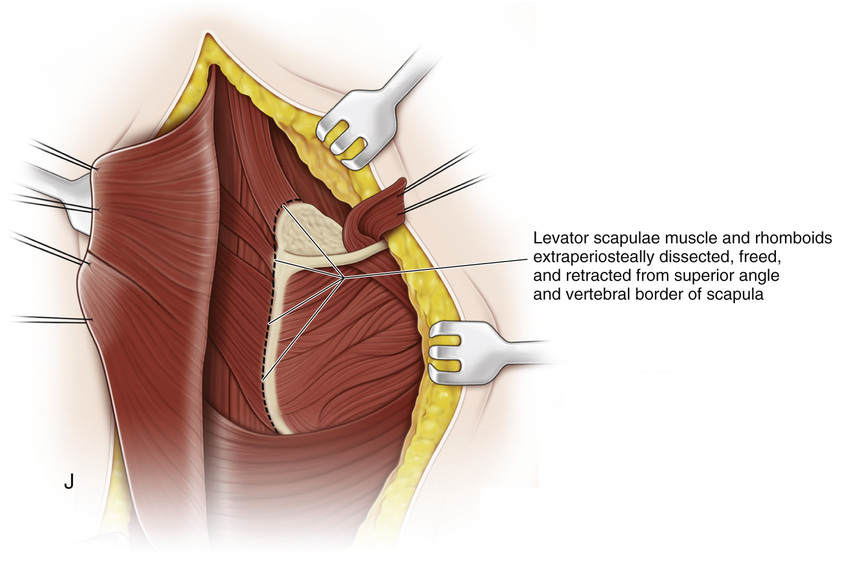
J, The insertion of the levator scapulae muscle on the superior angle of the scapula and the insertions of the rhomboideus muscles, major and minor, on the medial border of the scapula are extraperiosteally dissected, divided, and retracted, and their free ends are marked with 2-0 Mersilene suture.
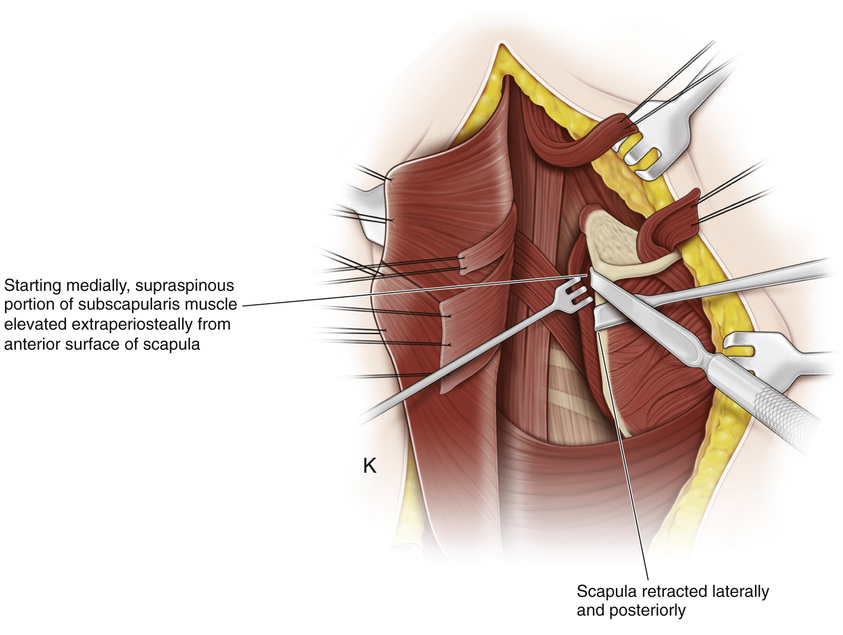
K, The superior margin of the scapula is then retracted posteriorly, and starting medially, the supraspinous portion of the subscapularis muscle is elevated extraperiosteally from the anterior surface of the scapula.
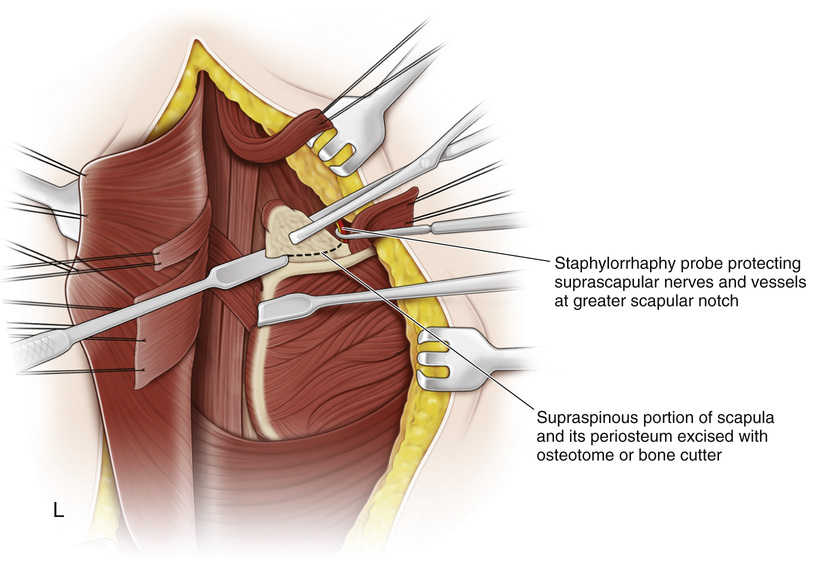
L, Next, a staphylorrhaphy probe is placed in the scapular notch to protect the suprascapular nerves and vessels, and with bone-cutting forceps or an osteotome, the supraspinous part of the scapula along with its periosteum is excised. (Currently, this author preserves the normal anatomy of the scapula because its supraspinous portion is often tilted anteriorly toward the rib cage, in which case a greenstick fracture is produced and the tilted portion elevated.)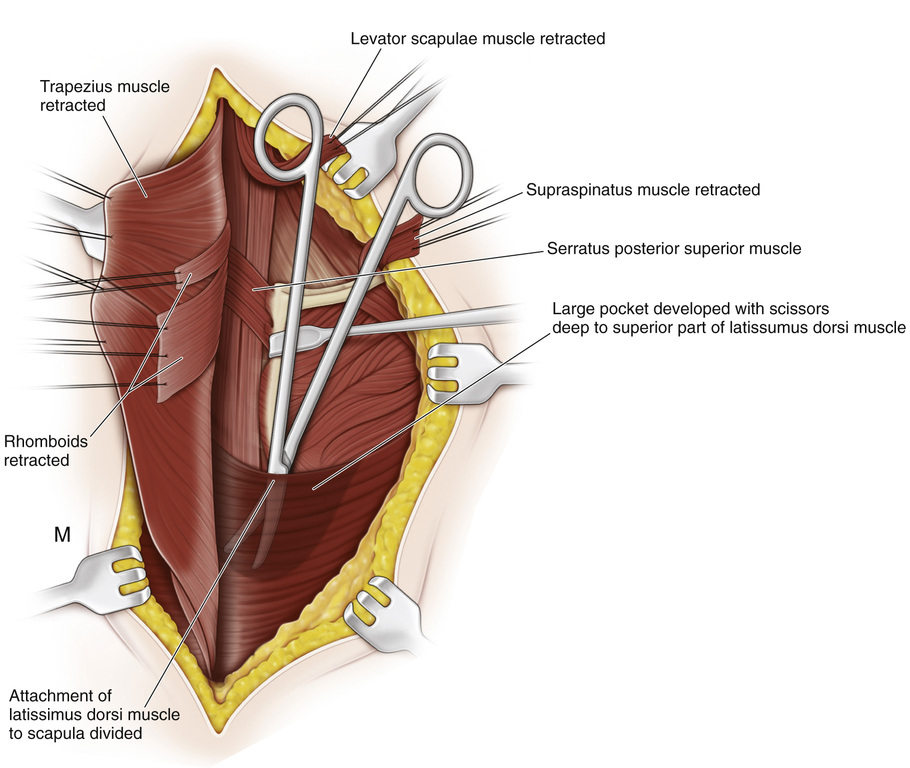
M, The attachments of the latissimus dorsi muscle to the scapula are then divided extraperiosteally, and by blunt dissection a large pocket is created deep to the superior part of the latissimus dorsi muscle.
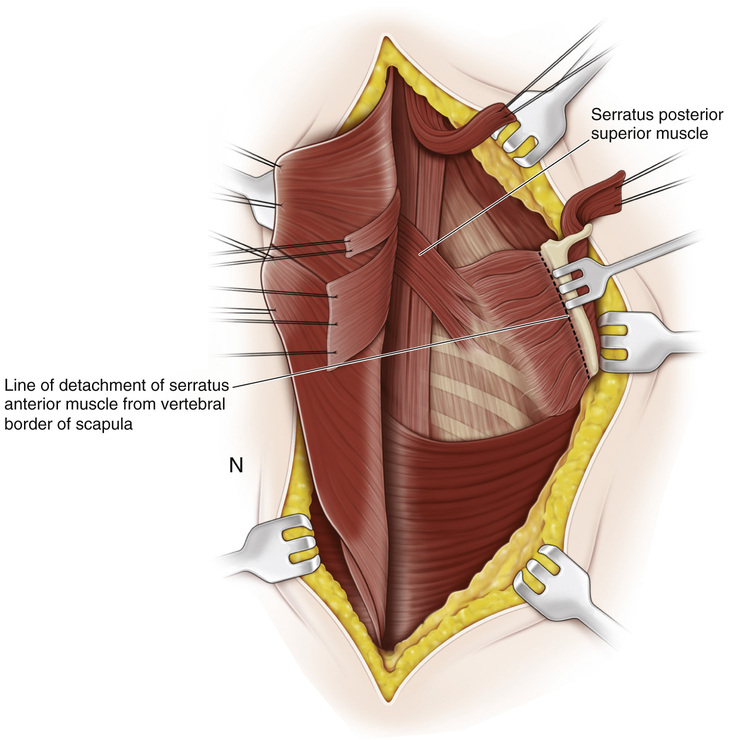
N, The medial border of the scapula is everted by retracting it posteriorly and laterally, and the insertions of the serratus anterior muscle to the vertebral margin and to the angle of the scapula are freed extraperiosteally and marked with 2-0 Mersilene suture.
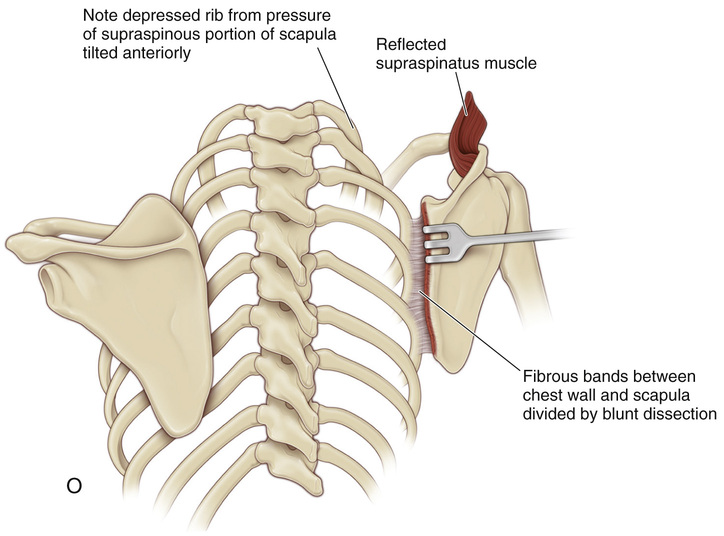
O, Thick fibrous bands may connect the scapula to the chest wall. They should be divided to mobilize the scapula so that it can be displaced distally enough.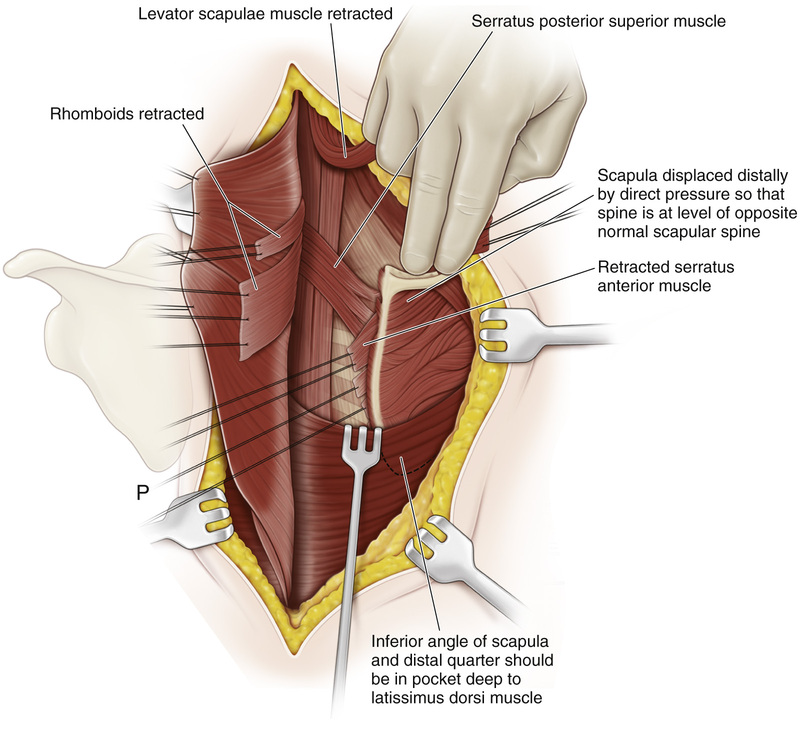
P, Then, by direct pressure and without traction on the arm, the scapula is gently displaced distally to the desired position. The possibility of stretching and damaging the brachial plexus must always be kept in mind, and vigorous manipulations should be avoided. The inferior angle and distal quarter of the scapula should be in the large pocket deep to the superior part of the latissimus dorsi muscle.
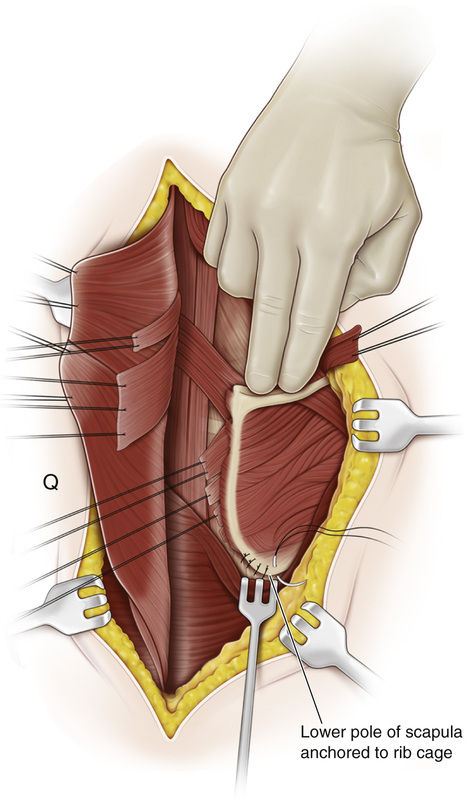
Q, If winging of the scapula is present, the inferior pole of the scapula is attached to the adjacent rib with two or three absorbable sutures. If the rhomboid muscles and other scapulocostal muscles are hypoplastic or fibrotic and marked winging of the scapula is noted, this author recommends fixing the scapula on the rib cage in a lowered and more laterally rotated position. The winging will be corrected, and the laterally rotated fixed position of the scapula will enable the patient to abduct the shoulder fully at the glenohumeral joint.
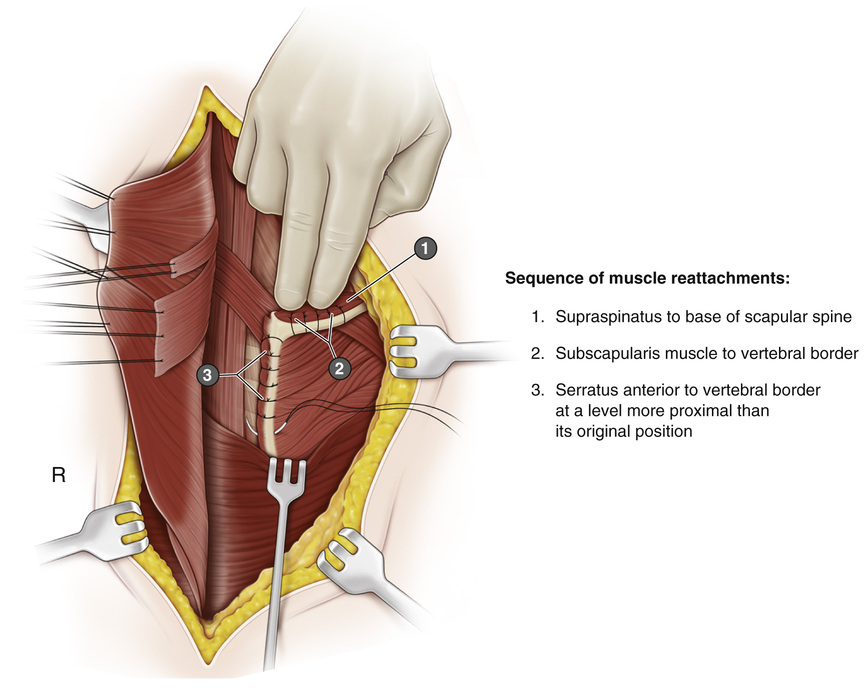
R, Next, while the assistant holds the scapula in its lowered position, the divided and marked muscles are reattached in the following order: (1) the supraspinatus to the base of the scapular spine, (2) the subscapularis to the vertebral border, and (3) the serratus anterior to the vertebral border at a level more proximal than its original position.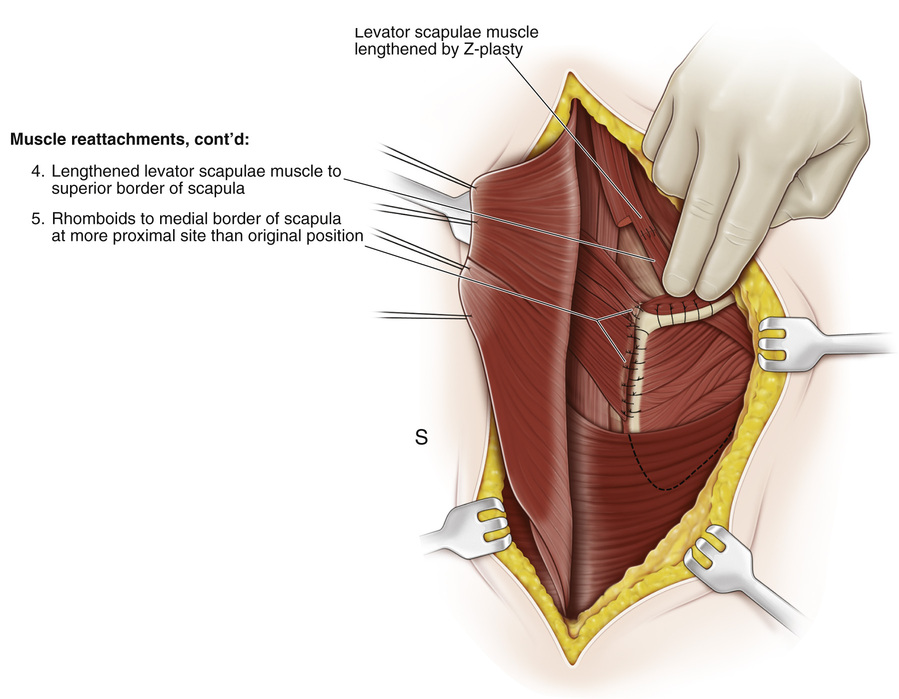
S, (4) The levator scapulae muscle, lengthened if necessary, is attached to the superior border of the scapula. (5) The rhomboids are attached to the medial border of the scapula at a more proximal site than the original position.
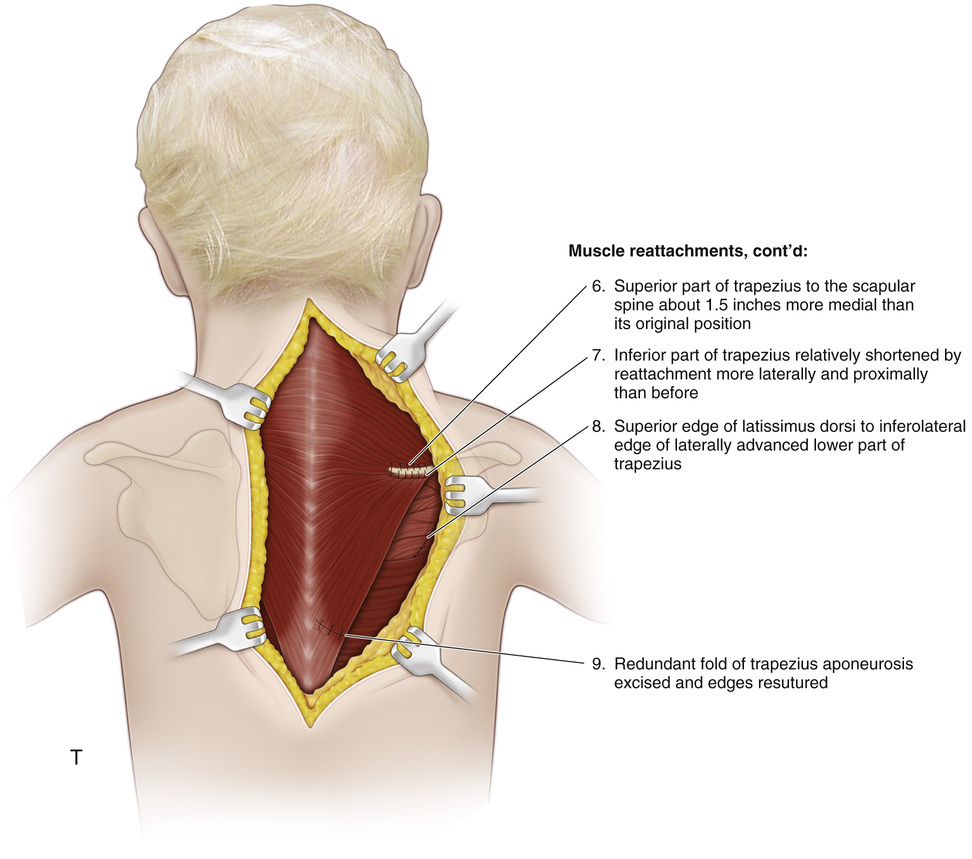
T, (6) The superior part of the trapezius is reattached to the scapular spine about  inches medial to its original position. (7) The inferior part of the trapezius is attached to the spine of the scapula more laterally and proximally than before. (8) The superior edge of the latissimus dorsi is attached to the inferolateral edge of the laterally advanced lower part of the trapezius. In the distal part of the incision, the origin of the lower part of the trapezius is followed, excess tissue is excised, and the free muscle edges are overlapped and sutured. The increased tension in this part of the muscle will serve as an added measure to hold the scapula in its lowered position. The wound is closed in layers. Closure of the skin should be subcuticular. If an associated pterygium colli is present, a Z-plasty repair may be performed.
inches medial to its original position. (7) The inferior part of the trapezius is attached to the spine of the scapula more laterally and proximally than before. (8) The superior edge of the latissimus dorsi is attached to the inferolateral edge of the laterally advanced lower part of the trapezius. In the distal part of the incision, the origin of the lower part of the trapezius is followed, excess tissue is excised, and the free muscle edges are overlapped and sutured. The increased tension in this part of the muscle will serve as an added measure to hold the scapula in its lowered position. The wound is closed in layers. Closure of the skin should be subcuticular. If an associated pterygium colli is present, a Z-plasty repair may be performed.
Related posts:
 23 Hamstring Lengthening
26 Shelf Acetabular Augmentation
51 Correction of Hammer Toe by Resection and Arthrodesis of the Proximal Interphalangeal Joint
41 Sacro-Iliac Screws
31 Anterior Transfer of the Peroneus Longus Tendon to the Base of the Second Metatarsal
37 Scapulocostal Stabilization for Scapular Winging (Ketenjian Technique)
23 Hamstring Lengthening
26 Shelf Acetabular Augmentation
51 Correction of Hammer Toe by Resection and Arthrodesis of the Proximal Interphalangeal Joint
41 Sacro-Iliac Screws
31 Anterior Transfer of the Peroneus Longus Tendon to the Base of the Second Metatarsal
37 Scapulocostal Stabilization for Scapular Winging (Ketenjian Technique)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


