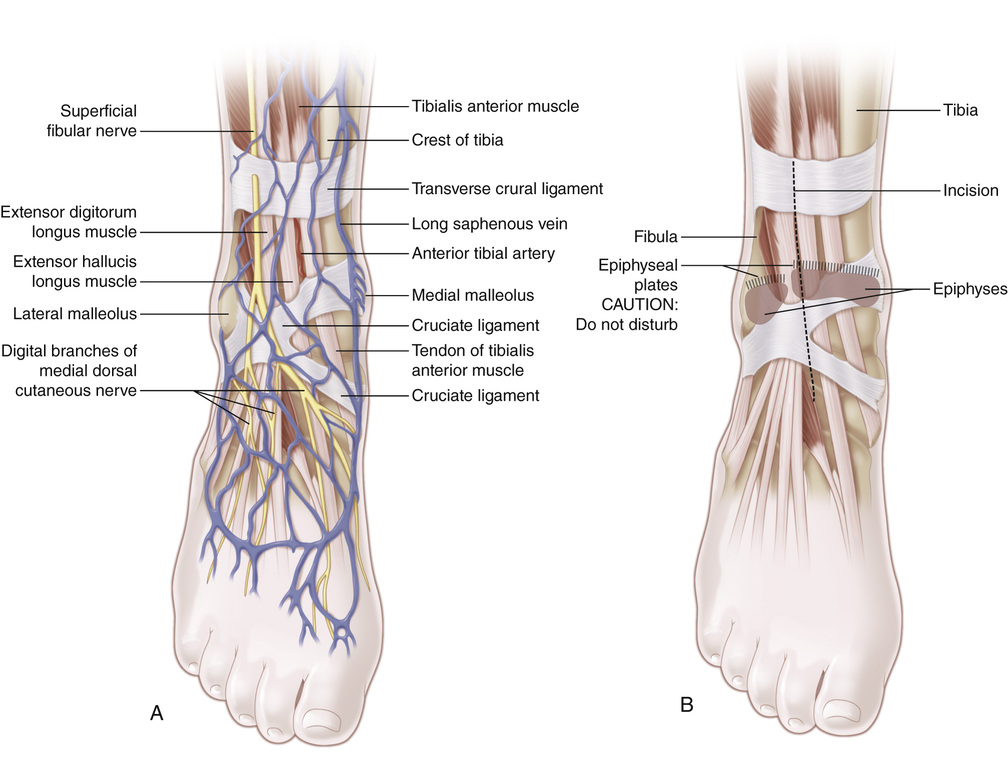
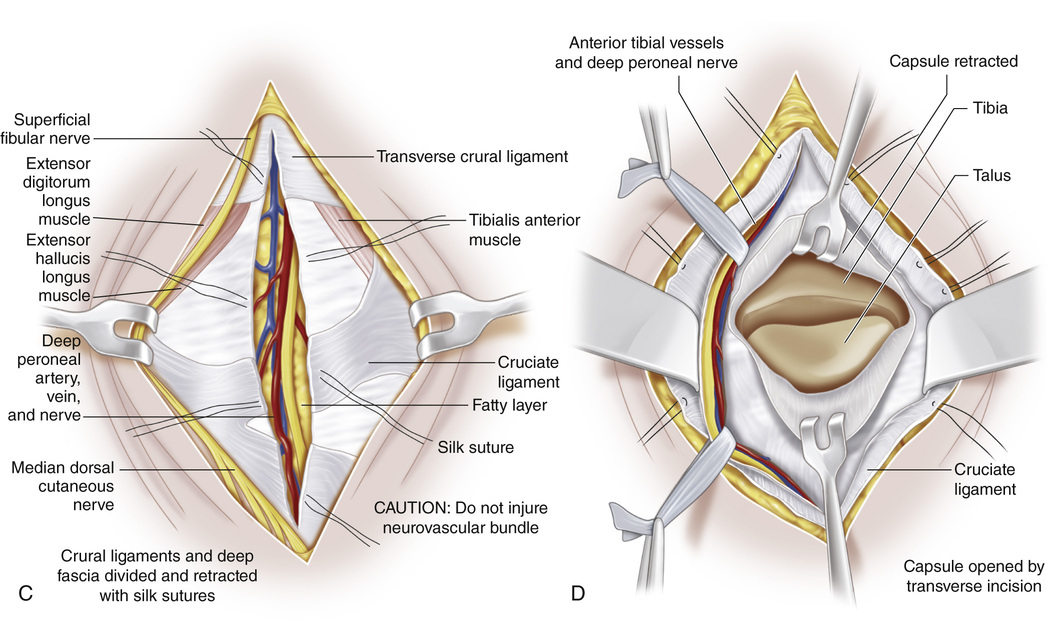
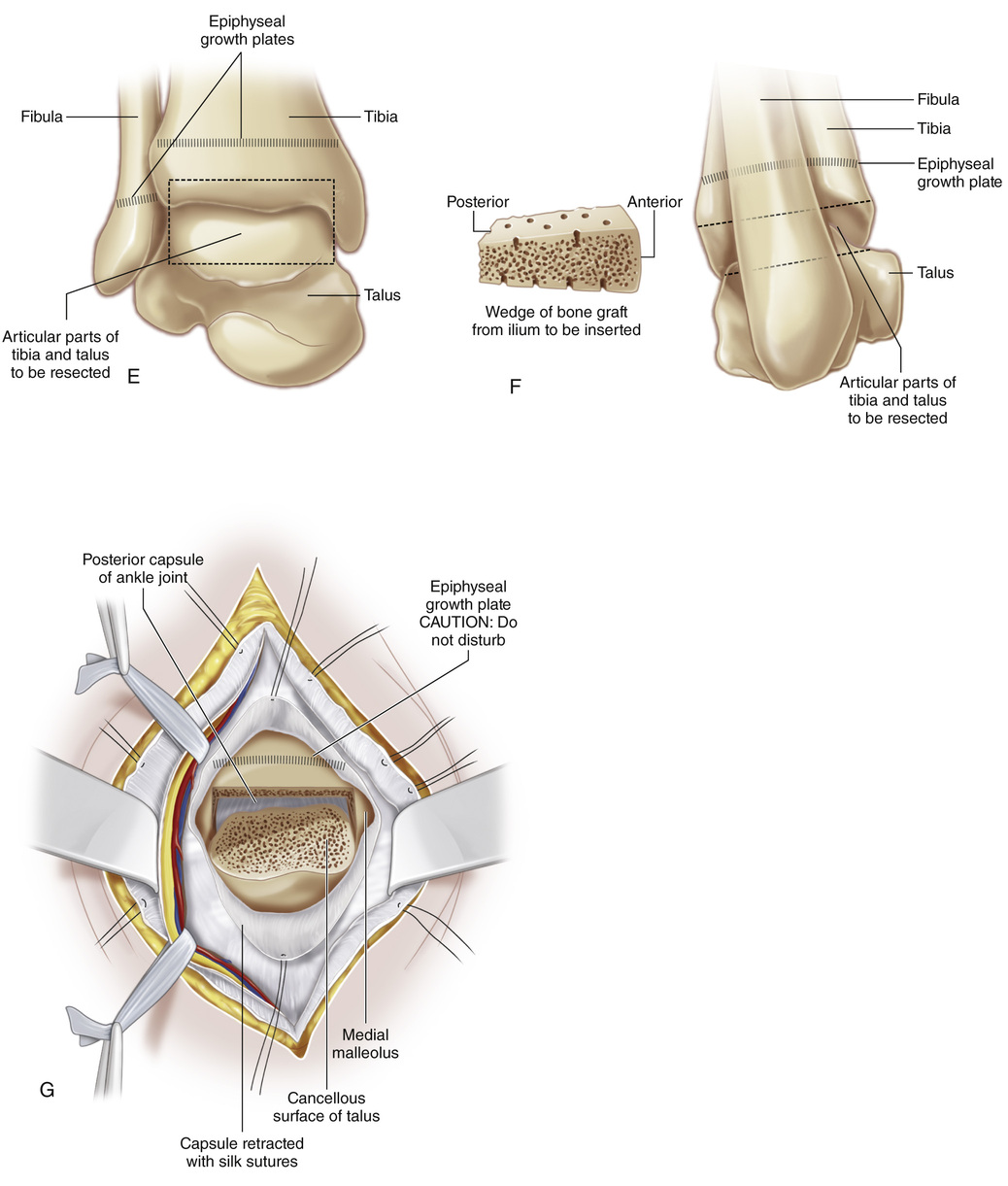
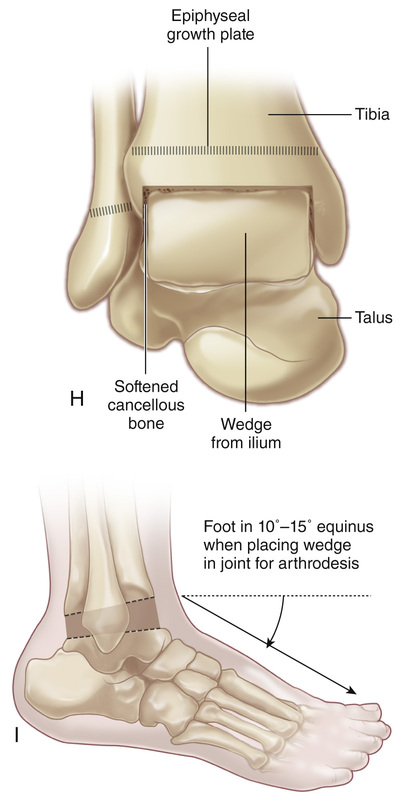
A and B, A longitudinal skin incision is made beginning 7 cm proximal to the ankle joint between the extensor digitorum longus and extensor hallucis longus tendons and extended distally across the ankle joint in line with the third metatarsal; the incision ends 4 cm distal to the ankle joint. The subcutaneous tissue is divided and the skin flaps are mobilized and retracted to their respective sides. The veins crossing the field are clamped, divided, and coagulated. The intermediate and medial dorsal cutaneous branches of the superficial peroneal nerve are identified and protected by retraction to one side of the wound. C, The deep fascia and transverse crural and cruciate crural ligaments are divided in line with the skin incision. The ligaments are marked with 00 silk suture for accurate closure later. D, The neurovascular bundle (deep peroneal nerve, anterior tibial–dorsalis pedis vessels) is identified, isolated, and retracted laterally with the extensor hallucis longus, extensor digitorum longus, and peroneus tertius tendons. The anterolateral malleolar and lateral tarsal arteries are isolated, clamped, divided, and ligated. The distal end of the tibia, ankle joint, and talus are identified. A transverse incision is made in the capsule of the talotibial joint from the posterior tip of the medial malleolus to the lateral malleolus. The edges of the capsule are marked with 00 silk suture for meticulous closure later. E to G, The capsule is reflected and retracted distally on the talus and proximally on the tibia. The periosteum of the tibia should not be divided. The distal tibial and fibular epiphyseal plates should not be disturbed in growing children. With thin curved and straight osteotomes, the cartilage and subchondral bone are removed from the opposing articular surfaces of the distal tibia and proximal talus down to raw bleeding cancellous bone. Cartilage chips should not be left posteriorly. H, Next a large piece of bone for grafting is taken from the ilium and fashioned to fit snugly in the ankle joint. The graft should have both cortices intact and should be thicker at one end and wedge shaped. The cortices of the graft are perforated with multiple tiny drill holes. The ankle joint is held in the desired position, and the bone graft is firmly fitted into the joint with an impactor. If any space is left on each side of the graft, it is packed with cancellous bone from the ilium. The graft in the ankle joint gives compression force to the arthrodesis and adds to the height of the foot and ankle. The capsule of the ankle joint and the transverse crural and cruciate crural ligaments are closed carefully in layers. The deep fascia and the wound are closed in the usual manner. Anteroposterior and lateral radiographs are taken to ensure that the ankle joint is in the desired position. I, A long-leg cast is applied with the ankle joint in the desired position of plantar flexion (boys, 10 degrees; girls, 15 to 20 degrees) and the knee in 45 degrees of flexion.
Arthrodesis of the Ankle Joint via the Anterior Approach Without Disturbing the Distal Tibial Growth Plate
Operative Technique
Related posts:
 23 Hamstring Lengthening
23 Hamstring Lengthening
 29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
 10 Pemberton Osteotomy
10 Pemberton Osteotomy
 33 Triple Arthrodesis
33 Triple Arthrodesis
 38 Exposure of the Spine for Posterior Instrumentation and Fusion
38 Exposure of the Spine for Posterior Instrumentation and Fusion
 42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


