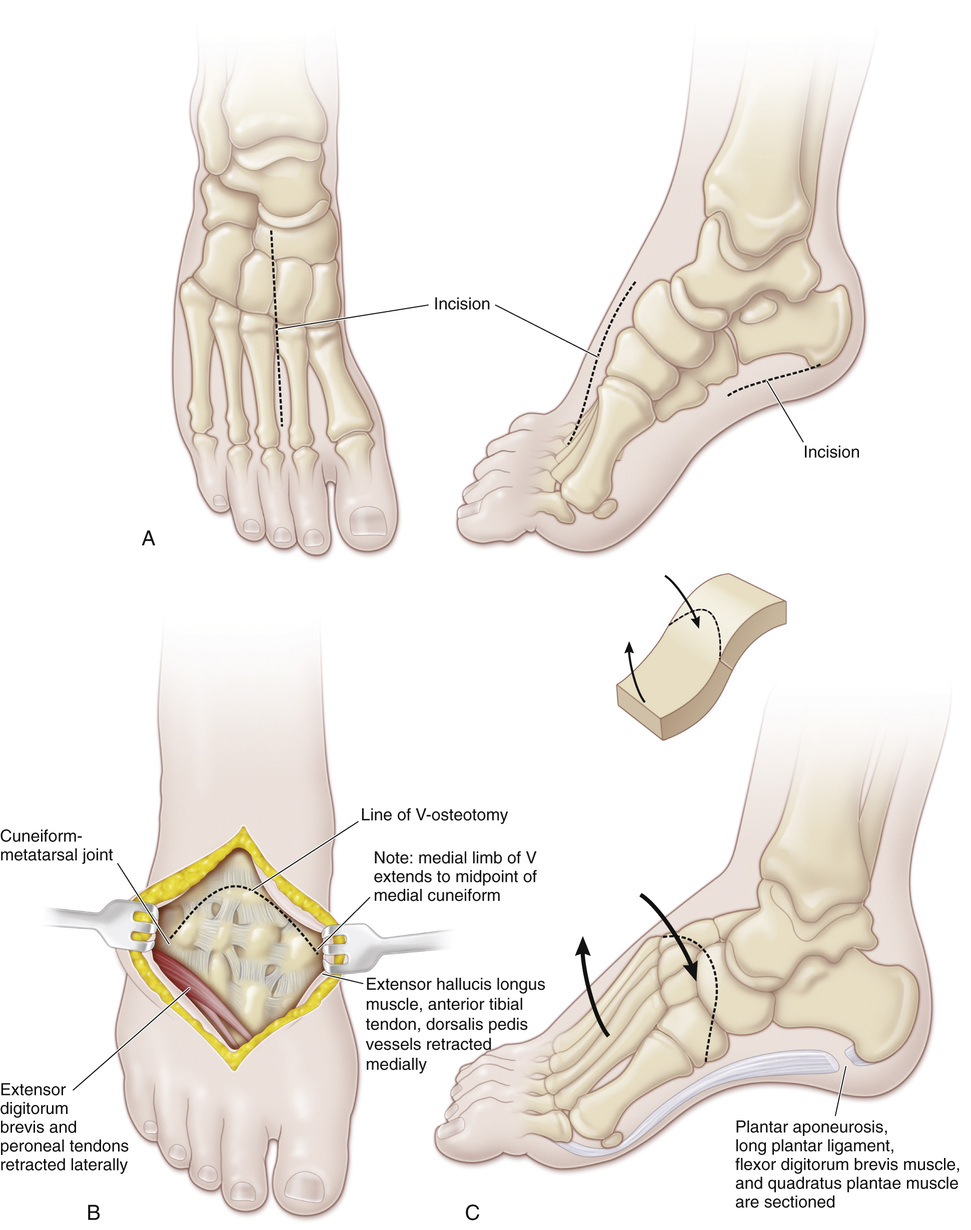
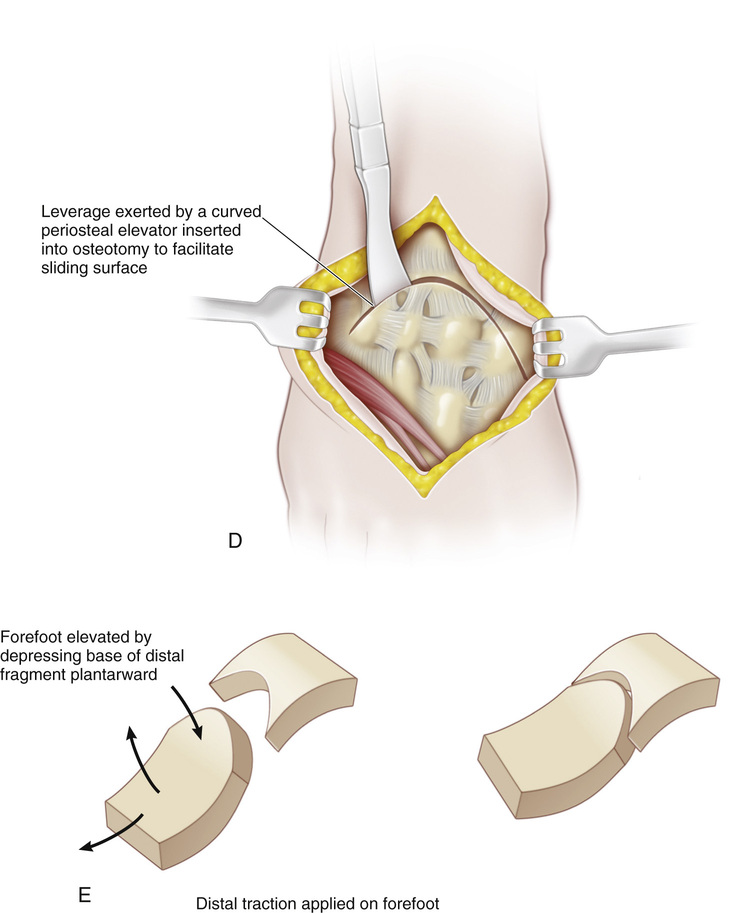
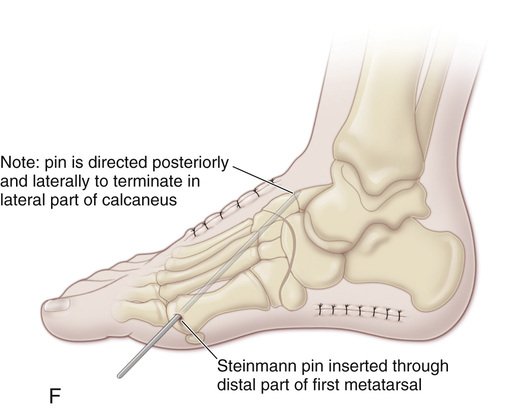
A, The dorsal aspect of the tarsal bones is exposed through a longitudinal incision 6 to 8 cm long in the midline of the foot (i.e., between the second and third rays) and centered over the midtarsal area at the naviculocuneiform junction. B and C, The subcutaneous tissue is divided. The superficial nerves are isolated and protected. The long toe extensor tendons are identified and separated, and the plane between those of the second and third toes is developed. The extensor digitorum brevis muscle is identified, elevated extraperiosteally, and retracted laterally with the peroneal tendons. The extensor hallucis longus tendon, dorsalis pedis vessels, and anterior tibial tendon are identified, dissected free, and retracted medially. The osteotomy site is exposed extraperiosteally. The talonavicular joint is identified next. Caution! Do not injure the midtarsal joint and compromise its function. If bony landmarks are distorted, radiographs are obtained for proper orientation. Inadvertent partial ostectomy of the head of the talus will result in aseptic necrosis and traumatic arthritis. The V line of the osteotomy is marked. Its apex is in the midline of the foot at the height of the arch of the cavus deformity, its medial limb extends to the middle of the medial cuneiform and exits proximal to the cuneiform–first metatarsal joint, and its lateral limb extends to the middle of the cuboid and emerges proximal to the cuboid–fifth metatarsal joint. Often the V is shallow, shaped more like a dome. D and E, The osteotomy is begun with an oscillating bone saw and completed with an osteotome. Splintering of the ends of the medial and lateral limbs should be avoided. Next, a curved periosteal elevator is inserted into the osteotomy site, manual traction is applied on the forefoot, and with the elevator used as a lever, the base of the distal fragment is depressed plantarward. This maneuver corrects the cavus deformity and lengthens the concave plantar surface of the foot. The foot is not shortened as it would be by resection of a bone wedge, and any abduction or adduction deformity can be corrected if necessary. F, Once the desired alignment is achieved, a single Steinmann pin is inserted through the distal part of the first metatarsal and directed posteriorly and laterally to terminate in the lateral part of the calcaneus or the cuboid. Radiographs are obtained to verify the completeness of correction. The tourniquet is then removed, hemostasis is achieved, and the wound is closed with interrupted sutures. The pin is cut subcutaneously, and a below-knee cast is applied.
Japas V-Osteotomy of the Tarsus
Operative Technique
Related posts:
 23 Hamstring Lengthening
23 Hamstring Lengthening
 29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
 10 Pemberton Osteotomy
10 Pemberton Osteotomy
 33 Triple Arthrodesis
33 Triple Arthrodesis
 38 Exposure of the Spine for Posterior Instrumentation and Fusion
38 Exposure of the Spine for Posterior Instrumentation and Fusion
 42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


