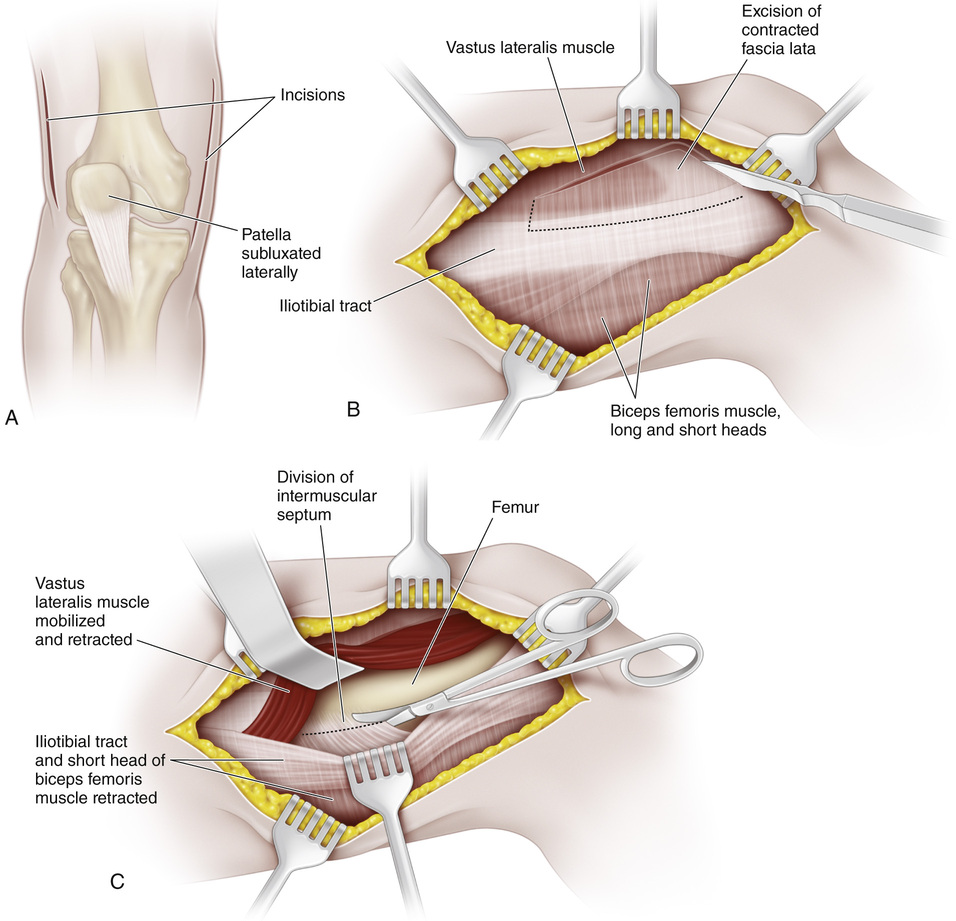
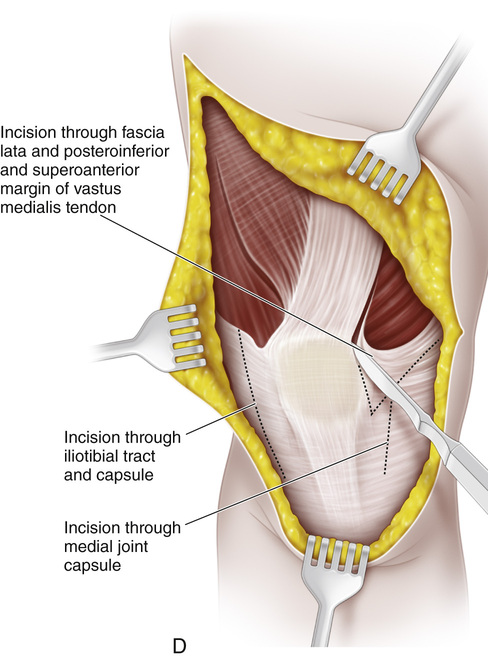
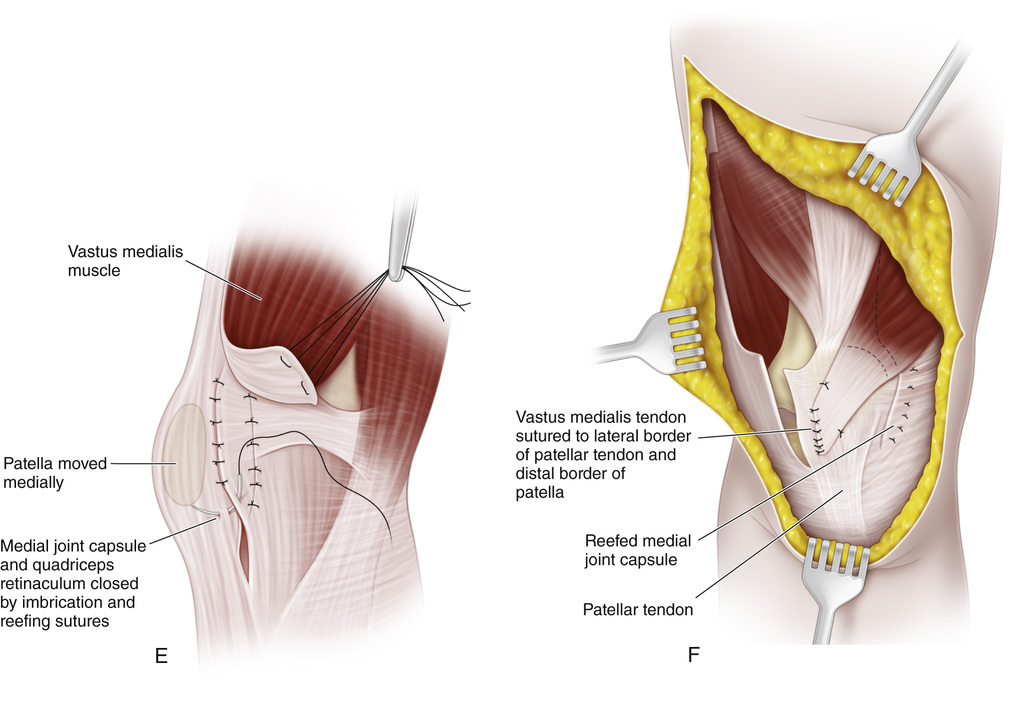
A, The surgical approach is through two longitudinal skin incisions. The first incision is medial, beginning 3 cm medial and 4 cm proximal to the superior pole of the patella and extending distally to terminate at a point 2 cm distal and 1 cm medial to the proximal tibial tubercle. The lateral longitudinal skin incision begins at the joint line 2 cm lateral to the lateral margin of the patellar tendon and extends proximally for a distance of 1 to 10 cm. In this drawing, a J-shaped incision is illustrated; we do not recommend its use because the operative scar is ugly. The subcutaneous tissue and superficial fascia are divided, and the skin flaps are developed medially and laterally to expose the quadriceps muscle, patella, patellar tendon, patellar retinaculum, joint capsule, and iliotibial band. B and C, Starting at a level 4 cm proximal to the lateral femoral condyle, a 7.5-cm segment of the fascia lata and the lateral intermuscular septum is excised. Next, abnormal attachments of the iliotibial band are divided, and the vastus lateralis muscle is widely mobilized from the deep surface of the fascia lata and its origin from the femur to allow free medial displacement of the patella. During this procedure, several muscular branches of the perforating arteries may be encountered, requiring coagulation or ligation. D and E, The contracted iliotibial tract, patellar retinaculum, and lateral joint capsule are then longitudinally divided in their posterolateral portion to allow medial displacement of the patella. The lax medial joint capsule and patellar retinaculum are longitudinally incised, to be reefed later. The insertion of the vastus medialis, with its tendinous fibers and the periosteum of the patella, is detached from the medial and superior border of the patella by U-shaped incisions in the superoanterior and posteroinferior margins of the muscle. The synovial membrane is not incised unless inspection of the interior of the joint for loose bodies or chondromalacia of the patella is indicated. Next, the patella is displaced medially and the medial joint capsule is imbricated and tightly closed by reefing sutures. With the knee in complete extension, the medial patellar retinaculum is also imbricated by reefing sutures. F, The superficial surface of the anterolateral third of the inferior half of the patella is then roughened with curved osteotomes and a curet. The vastus medialis tendon is transferred laterally and distally deep to the patellar bursa and sutured to the lateral border of the patellar tendon. The wounds are closed in layers and a well-molded cylinder cast is applied with the knee in neutral position or in 5 degrees of flexion.
Quadricepsplasty for Recurrent Dislocation of the Patella (Green Procedure)
Operative Technique
Related posts:
 23 Hamstring Lengthening
23 Hamstring Lengthening
 29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
 10 Pemberton Osteotomy
10 Pemberton Osteotomy
 64 Amputation Through the Arm
64 Amputation Through the Arm
 38 Exposure of the Spine for Posterior Instrumentation and Fusion
38 Exposure of the Spine for Posterior Instrumentation and Fusion
 42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


