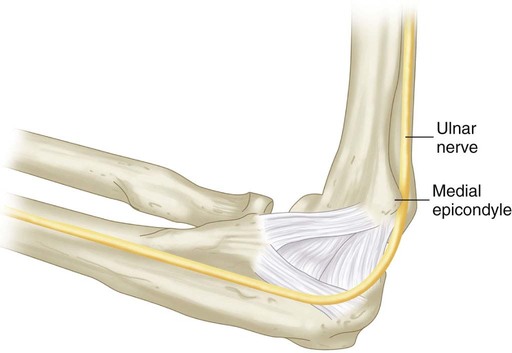
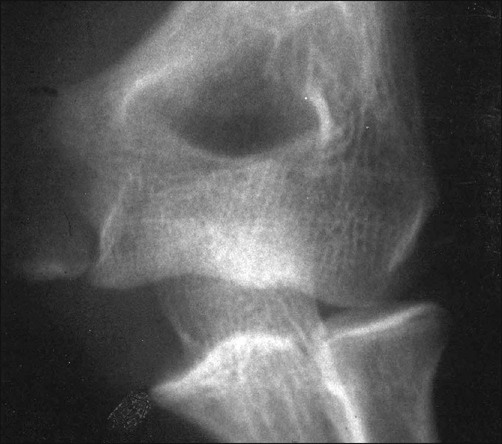
Pitfalls • Simple avulsion fractures, minimally displaced, can be treated nonoperatively (Bede et al., 1975). • If the AP radiograph demonstrates a minimally displaced fracture and the lateral radiograph does not demonstrate a fat pad sign, then a simple avulsion fracture (Fig. 1) has occurred rather than a fracture associated with an elbow dislocation or subluxation. • The AP radiograph is best for determining the amount of displacement of the medial epicondyle fracture (Fig. 2). • The lateral radiograph is examined to be certain that the elbow joint is reduced and that the medial epicondyle fragment is not in the joint (Fowles et al., 1984) (Fig. 3). • The valgus stress view (Fig. 4) can be utilized to demonstrate valgus instability of the elbow. This can be done prior to surgery with a gravity valgus stress test, or under anesthesia prior to making the skin incision (Case and Hennrikus, 1997; Schwab et al., 1980; Woods and Tullos, 1977).
Open Reduction and Internal Fixation of Displaced Medial Epicondyle Fracture Using a Screw and Washer
Indications
 An acute, displaced medial epicondyle fracture associated with an elbow dislocation or subluxation in an adolescent athlete
An acute, displaced medial epicondyle fracture associated with an elbow dislocation or subluxation in an adolescent athlete

Examination/Imaging
 The skin is examined for abrasions or open injuries.
The skin is examined for abrasions or open injuries.
 The wrist and shoulder are also examined for possible additional injuries.
The wrist and shoulder are also examined for possible additional injuries.
 Plain radiographs should be obtained in anteroposterior (AP), lateral, and valgus stress views.
Plain radiographs should be obtained in anteroposterior (AP), lateral, and valgus stress views.


Positioning
 Supine positioning is used, with a plexiglass radiolucent upper extremity table for the injured elbow (Fig. 6).
Supine positioning is used, with a plexiglass radiolucent upper extremity table for the injured elbow (Fig. 6).Related posts:
![]() 13: Triple Pelvic Osteotomy
13: Triple Pelvic Osteotomy
![]() 15: Repair of Proximal Hamstring Avulsion
15: Repair of Proximal Hamstring Avulsion
![]() 28: Femur Fracture: Closed Reduction and Spica Cast
28: Femur Fracture: Closed Reduction and Spica Cast
![]() 18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
![]() 47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


4: Open Reduction and Internal Fixation of Displaced Medial Epicondyle Fracture Using a Screw and Washer