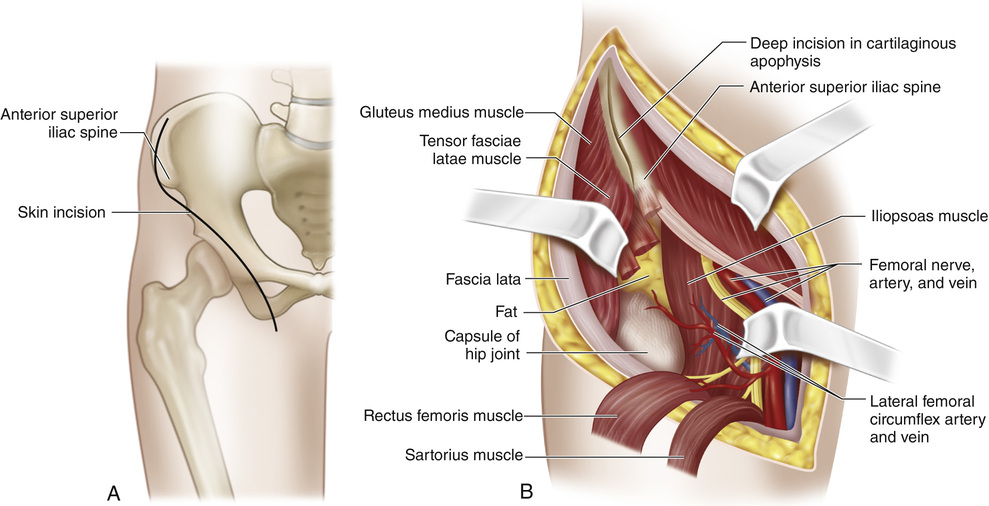
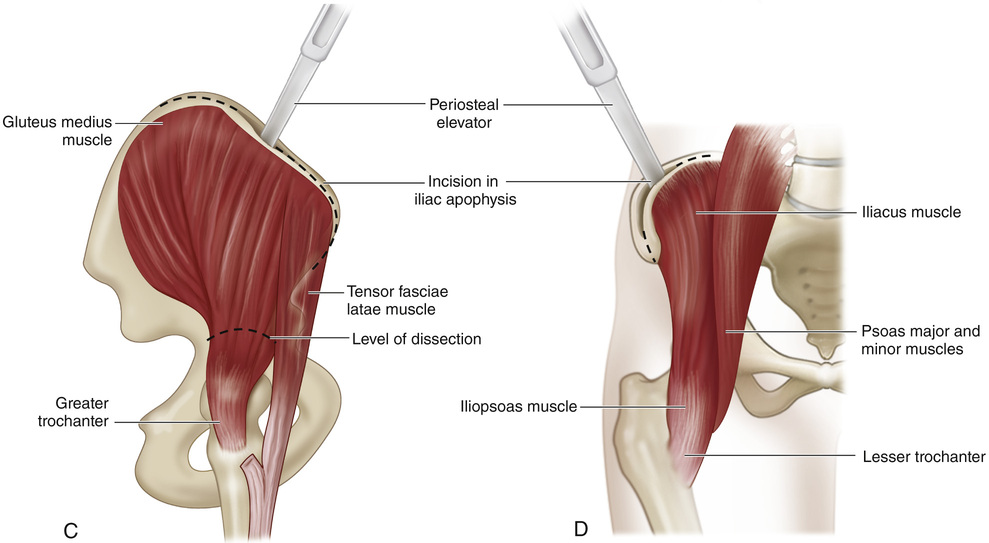
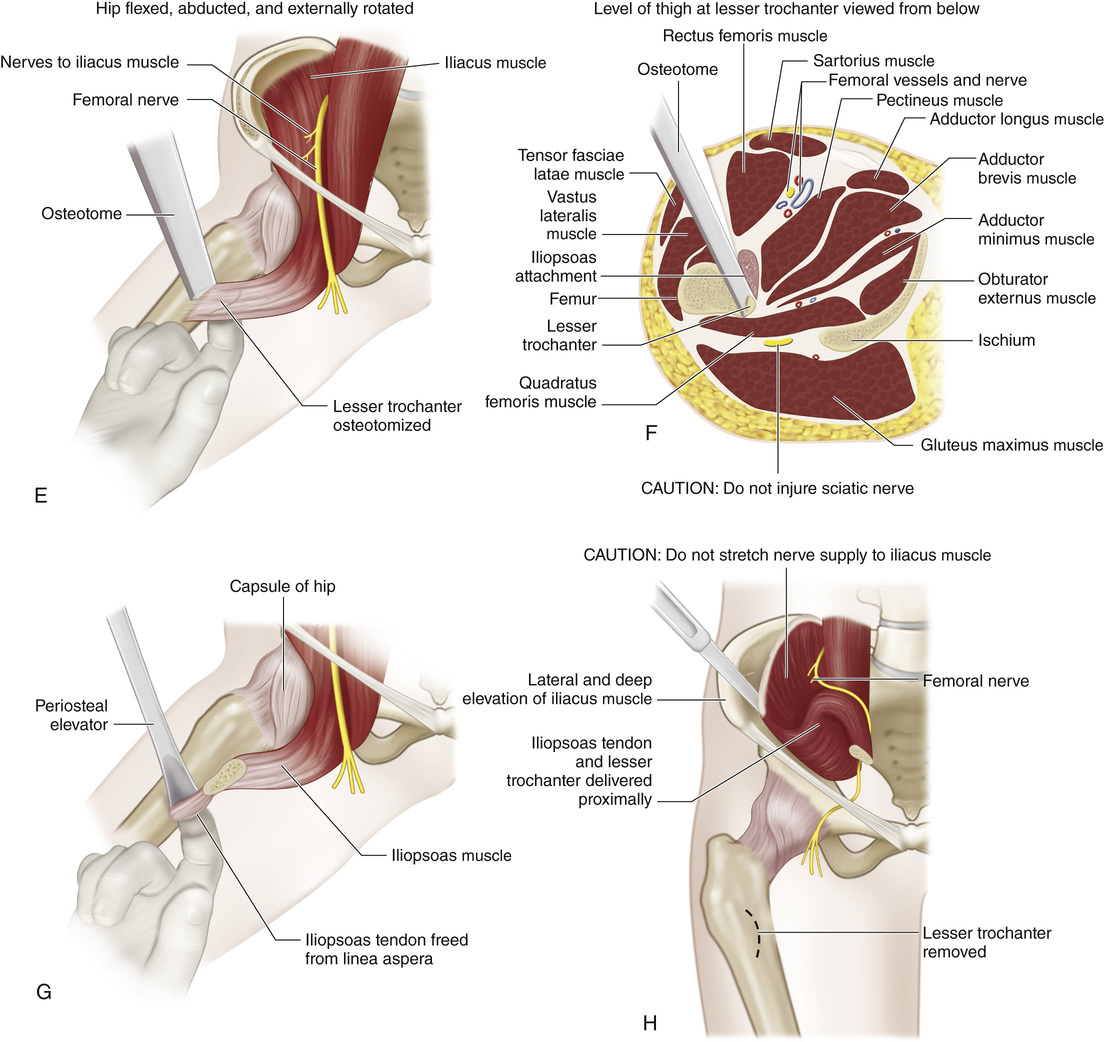
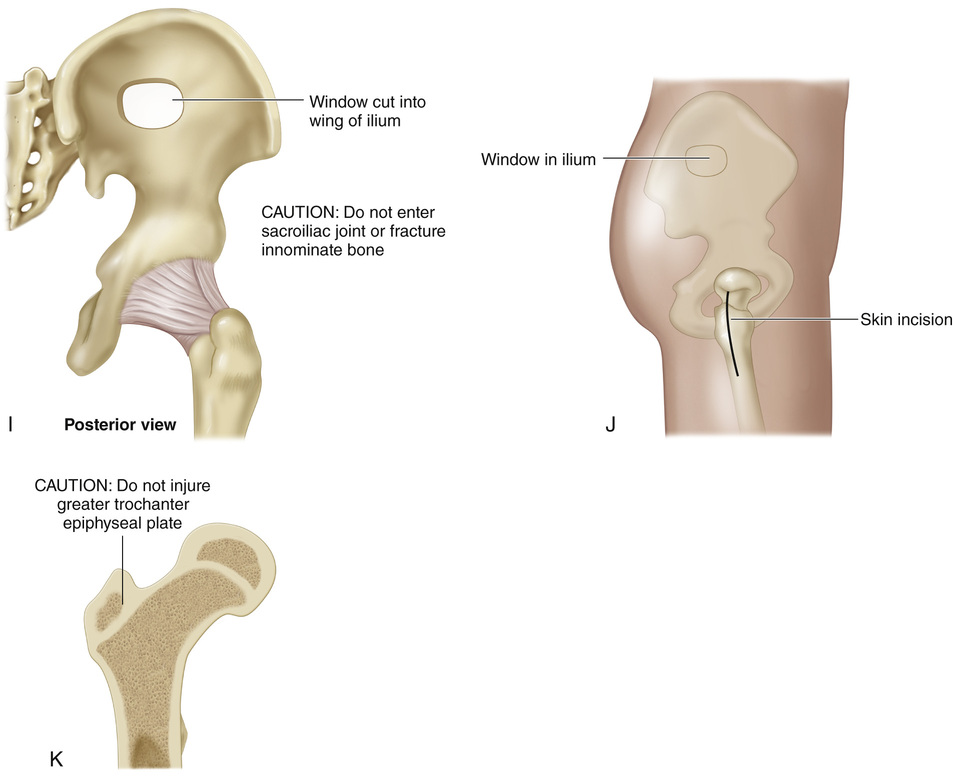
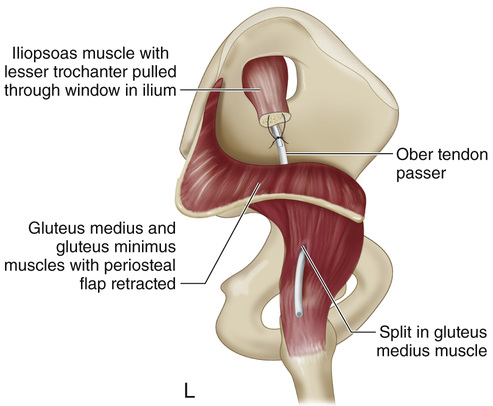
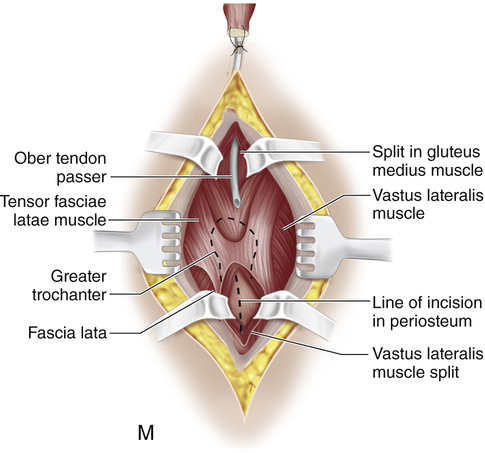
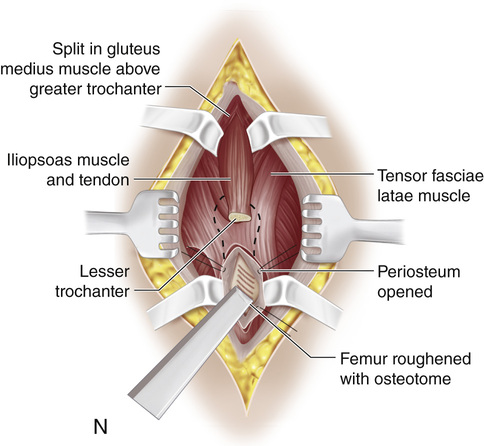
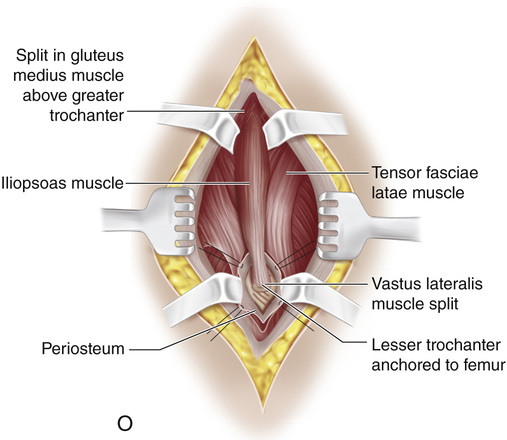
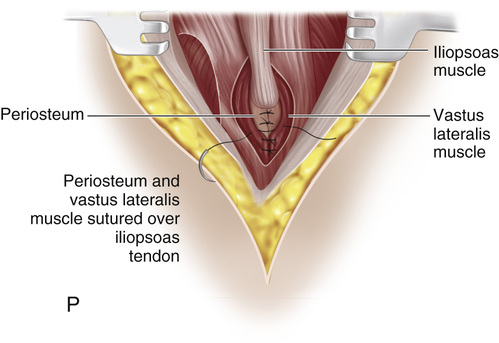
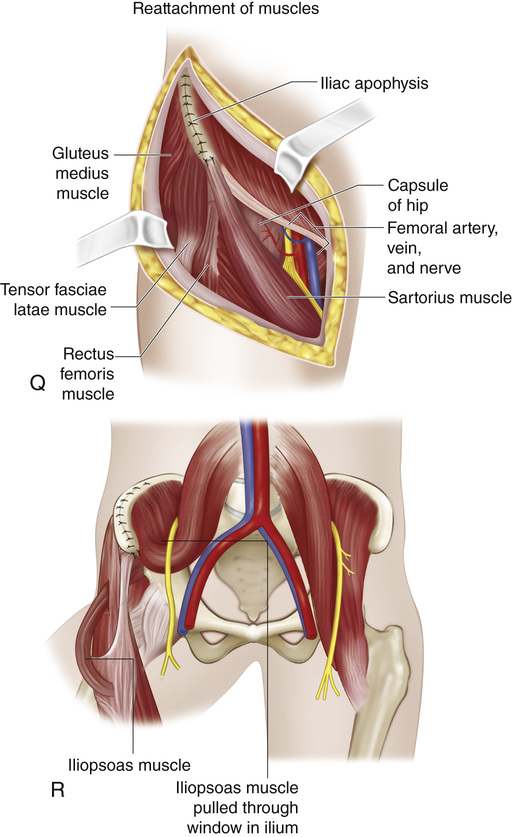
The patient is positioned supine with a small sandbag under the sacrum and a larger sandbag under the ipsilateral scapula. The entire involved lower limb, the hip, the lower part of the abdomen and chest, and the iliac and sacral regions are prepared in sterile fashion and draped so that the limb that is to be operated on can be freely manipulated and the incision extended to the posterior third of the iliac crest without contamination. A, The skin incision extends forward from the junction of the posterior and middle thirds of the iliac crest to the anterior superior iliac spine; it is then carried distally into the thigh along the medial border of the sartorius muscle for a distance of 10 to 12 cm and ends 2 cm distal to the lesser trochanter. B, The deep fascia is incised over the iliac crest, and the fascia lata is opened in line with the skin incision. The lateral femoral cutaneous nerve is identified; it usually crosses the sartorius muscle 2.5 cm distal to the anterior superior iliac spine and lies in close proximity to the lateral border of the sartorius. The nerve is mobilized by sharp dissection and protected by retracting it medially with moist hernia tape. The wound flaps are undermined and retracted. The anterior medial margin of the tensor fasciae latae muscle is identified, and by blunt dissection, the groove between the sartorius and rectus femoris muscles medially and the tensor fasciae latae muscle laterally is opened. The dissection is carried deep through the loose areolar tissue that separates these structures, and the adipose tissue that covers the front of the capsule of the hip joint is exposed. The ascending branch of the lateral femoral circumflex artery and the accompanying vein cross the midportion of the wound; they are isolated, clamped, cut, and ligated. The origin of the sartorius muscle from the anterior superior iliac spine is detached and the muscle is reflected distally and medially. The free end is marked with a silk whip suture for later reattachment. The origins of the two heads of the rectus femoris are divided and reflected distally. The femoral nerve and its branches to the sartorius and rectus femoris are identified. Moist hernia tape is passed around the femoral nerve for gentle handling. The femoral vessels and nerve are retracted medially. C, The cartilaginous apophysis of the ilium is split and the dissection is deepened along the iliac crest down to bone. With a broad periosteal elevator the tensor fasciae latae and the gluteus medius and minimus muscles are stripped subperiosteally from the lateral surface of the ilium and reflected in one continuous mass laterally and distally to the superior margin of the acetabulum. Bleeding is controlled by packing the interval between the reflected muscles and ilium with laparotomy pads. D, Then, with a large periosteal elevator, the iliacus muscle is subperiosteally elevated and reflected medially to expose the inner wall of the wing of the ilium from the greater sciatic notch to the anterior superior iliac spine. By careful blunt dissection with a periosteal elevator, the iliacus muscle is freed, elevated, and mobilized from the inner wall of the ilium and the anterior capsule of the hip joint. It is important to stay lateral and deep to the iliacus muscle and work in a proximal-to-distal direction. E to G, Next the hip is flexed, abducted, and laterally rotated, and with the index finger the lesser trochanter is cleared of soft tissues proximally, posteriorly, and distally. The index finger is then placed on the posteromedial aspect of the lesser trochanter and is used to direct a curved osteotome to the superior and deep aspect of the base of the lesser trochanter. The lesser trochanter is osteotomized and the distal insertion of the iliacus muscle on the linea aspera of the femur is freed with a periosteal elevator. H, The iliacus and psoas muscles are reflected proximally by sharp and dull dissection. It is essential to avoid injuring the nerve to the iliacus, which at times enters the muscle belly distally; in addition, the femoral nerve should not be damaged. We find the use of a nerve stimulator of great help. Circumflex vessels are clamped, cut, and ligated as necessary. I, In the middle third of the wing of the ilium a rectangular hole, usually 1 to 2 in, is cut with drill holes and osteotomes. The hole should be large enough to accommodate the transferred muscle. It should be located as far posteriorly as possible to allow a more direct line of muscle action. The limiting factor is the nerve supply to the iliacus, which should not be stretched. J, With the hip in extension and medial rotation, the greater trochanter is exposed via a longitudinal lateral incision. The vastus lateralis muscle is split and the lateral surface of the proximal 4 to 5 cm of femoral shaft is subperiosteally exposed. K, It is important to avoid damaging the apophyseal growth plate of the greater trochanter. L, Next a large Ober tendon passer is inserted through the hole in the wing of the ilium, directed deep to the glutei, and brought out in the greater trochanteric region by splitting the insertion of the fibers of the gluteus medius muscle. M and N, The iliopsoas muscle is then transferred laterally by this route with the Ober tendon passer. The nerve supply to the iliacus is again checked to be sure that it is not under great tension. Next the hip is abducted at least 45 to 60 degrees and internally rotated 10 to 15 degrees. The site of insertion of the iliopsoas tendon on the femoral shaft is determined and roughened with curved osteotomes. The muscle should be under proper tension. O, The lesser trochanter is anchored to the proximal end of the femur by one or two transversely placed small staples. Mustard recommends making a trapdoor in the femur, into which the lesser trochanter is drawn and anchored by heavy wire sutures. P, The periosteum and vastus lateralis muscle are sutured to the edges and over the iliopsoas tendon. Q and R, The rectus femoris and sartorius muscles are sutured to the inferior and superior iliac spines, respectively. The tensor fasciae latae, gluteus medius and minimus, and abdominal muscles are sutured to the iliac crest. The wound is closed in layers in routine manner. A one-and-one-half hip spica cast is applied with the hip in 60 degrees of abduction, 10 to 15 degrees of medial rotation, and slight flexion.
Iliopsoas Muscle Transfer for Paralysis of the Hip Abductors
Operative Technique
Related posts:
 23 Hamstring Lengthening
26 Shelf Acetabular Augmentation
51 Correction of Hammer Toe by Resection and Arthrodesis of the Proximal Interphalangeal Joint
41 Sacro-Iliac Screws
31 Anterior Transfer of the Peroneus Longus Tendon to the Base of the Second Metatarsal
37 Scapulocostal Stabilization for Scapular Winging (Ketenjian Technique)
23 Hamstring Lengthening
26 Shelf Acetabular Augmentation
51 Correction of Hammer Toe by Resection and Arthrodesis of the Proximal Interphalangeal Joint
41 Sacro-Iliac Screws
31 Anterior Transfer of the Peroneus Longus Tendon to the Base of the Second Metatarsal
37 Scapulocostal Stabilization for Scapular Winging (Ketenjian Technique)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


