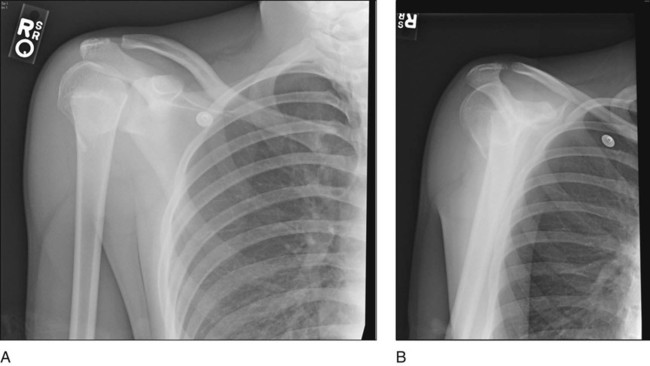
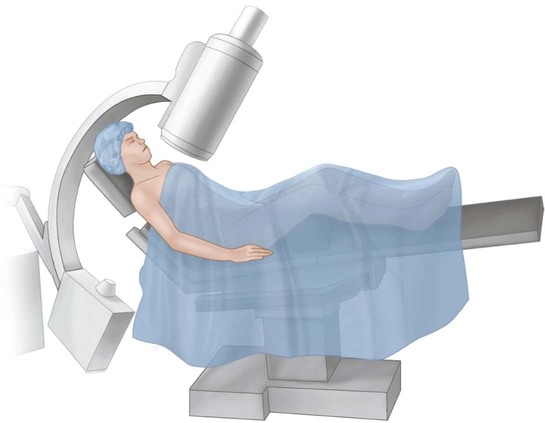
PROCEDURE 3 Proximal Humerus Fracture Reduction and Fixation with Elastic Nail Jay C. Albright Indications Significantly displaced proximal humeral physeal fracture in an older adolescent (2 or less years of growth remaining) Closed injury No distal trauma (ipsilateral elbow fractures) Pitfalls • Younger patients will likely remodel, and no surgery may be necessary other than closed reduction or hanging arm cast. • Premature growth arrest may limit the amount of remodeling potential and limit a patient’s ability to return to full function (overhead athletes). Controversies • Patients with more than 2–3 years of growth remaining will likely remodel adequately even in displaced fractures, provided no growth arrest occurs. Examination/Imaging Adequate anteroposterior (AP) (Fig. 1A) and orthogonal radiographs, either an axillary lateral or a scapular Y view (Fig. 1B), are needed to visualize the position of the fracture. FIGURE 1 Treatment Options • Closed reduction with percutaneous pin fixation • Closed reduction with percutaneous screw fixation • Open reduction and internal fixation Surgical Anatomy This procedure uses a lateral epicondylar approach to the distal humerus. The radial nerve is at risk from excessive dissection proximally or anteriorly. The extensor origins are at risk distally, inserting onto the epicondyle. Positioning The beach chair position can be used with relative ease, allowing for adequate fluoroscopic imaging (Fig. 2). FIGURE 2 Pearls • Ensure that adequate radiographic images can be obtained in both a true AP and an axillary lateral view. • Rotate the image intensifier to obtain the orthogonal views. • Use standard padding for all extremities. • Beach chair positioning can facilitate reduction with the help of gravity. Pitfalls • Neutral head position is absolutely necessary. Equipment • The fluoroscope should enter from the cephalad end of the room. • The operating table should be turned to accommodate this position. Controversies Only gold members can continue reading. Log In or Register to continue Share this:Click to share on Twitter (Opens in new window)Click to share on Facebook (Opens in new window) Related Related posts: 50: Flexor Tenotomy for Congenital Curly Toe 20: Anteromedial Approach to a Developmentally Dislocated Hip 28: Femur Fracture: Closed Reduction and Spica Cast 46: Resection of Talocalcaneal Tarsal Coalition and Fat Autograft Interposition 57: Scoliosis Correction 10: Digital Syndactyly Release Stay updated, free articles. Join our Telegram channel Join Tags: Operative Techniques Pediatric Orthopaedic Surgery Jun 7, 2016 | Posted by admin in ORTHOPEDIC | Comments Off on 3: Proximal Humerus Fracture: Reduction and Fixation with Elastic Nail Full access? Get Clinical Tree
PROCEDURE 3 Proximal Humerus Fracture Reduction and Fixation with Elastic Nail Jay C. Albright Indications Significantly displaced proximal humeral physeal fracture in an older adolescent (2 or less years of growth remaining) Closed injury No distal trauma (ipsilateral elbow fractures) Pitfalls • Younger patients will likely remodel, and no surgery may be necessary other than closed reduction or hanging arm cast. • Premature growth arrest may limit the amount of remodeling potential and limit a patient’s ability to return to full function (overhead athletes). Controversies • Patients with more than 2–3 years of growth remaining will likely remodel adequately even in displaced fractures, provided no growth arrest occurs. Examination/Imaging Adequate anteroposterior (AP) (Fig. 1A) and orthogonal radiographs, either an axillary lateral or a scapular Y view (Fig. 1B), are needed to visualize the position of the fracture. FIGURE 1 Treatment Options • Closed reduction with percutaneous pin fixation • Closed reduction with percutaneous screw fixation • Open reduction and internal fixation Surgical Anatomy This procedure uses a lateral epicondylar approach to the distal humerus. The radial nerve is at risk from excessive dissection proximally or anteriorly. The extensor origins are at risk distally, inserting onto the epicondyle. Positioning The beach chair position can be used with relative ease, allowing for adequate fluoroscopic imaging (Fig. 2). FIGURE 2 Pearls • Ensure that adequate radiographic images can be obtained in both a true AP and an axillary lateral view. • Rotate the image intensifier to obtain the orthogonal views. • Use standard padding for all extremities. • Beach chair positioning can facilitate reduction with the help of gravity. Pitfalls • Neutral head position is absolutely necessary. Equipment • The fluoroscope should enter from the cephalad end of the room. • The operating table should be turned to accommodate this position. Controversies Only gold members can continue reading. Log In or Register to continue Share this:Click to share on Twitter (Opens in new window)Click to share on Facebook (Opens in new window) Related Related posts: 50: Flexor Tenotomy for Congenital Curly Toe 20: Anteromedial Approach to a Developmentally Dislocated Hip 28: Femur Fracture: Closed Reduction and Spica Cast 46: Resection of Talocalcaneal Tarsal Coalition and Fat Autograft Interposition 57: Scoliosis Correction 10: Digital Syndactyly Release Stay updated, free articles. Join our Telegram channel Join Tags: Operative Techniques Pediatric Orthopaedic Surgery Jun 7, 2016 | Posted by admin in ORTHOPEDIC | Comments Off on 3: Proximal Humerus Fracture: Reduction and Fixation with Elastic Nail Full access? Get Clinical Tree