Extraarticular Arthrodesis of the Subtalar Joint (Grice Procedure)
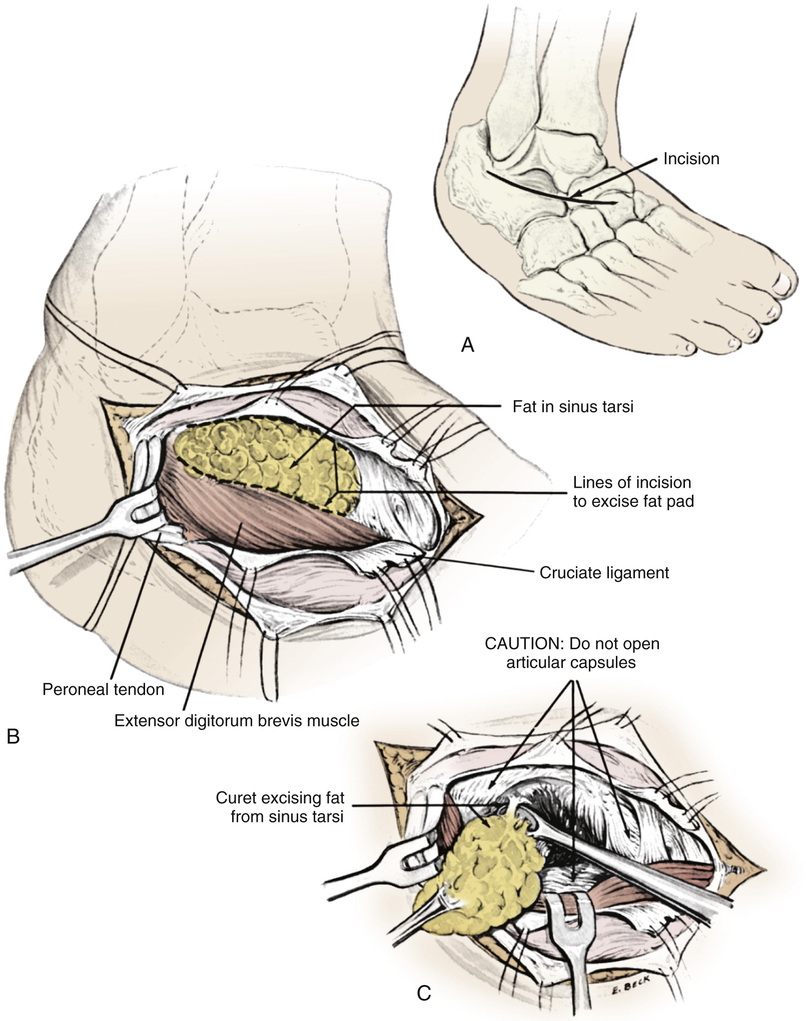
A, A  -inch-long, slightly curved incision is made over the subtalar joint, centered over the sinus tarsi.
-inch-long, slightly curved incision is made over the subtalar joint, centered over the sinus tarsi.
B, The incision is carried down to the sinus tarsi. The capsules of the posterior and anterior subtalar articulations are identified and left intact. The operation is extraarticular. If the capsule is inadvertently opened, it should be closed with interrupted sutures.
The periosteum on the talus corresponding to the lateral margin of the roof of the sinus tarsi is divided and reflected proximally. The fibrofatty tissue in the sinus tarsi and the tendinous origin of the short toe extensors from the calcaneus are elevated and reflected distally in one mass.
C, The remaining fatty and ligamentous tissue from the sinus tarsi is thoroughly removed with a sharp scalpel and curet.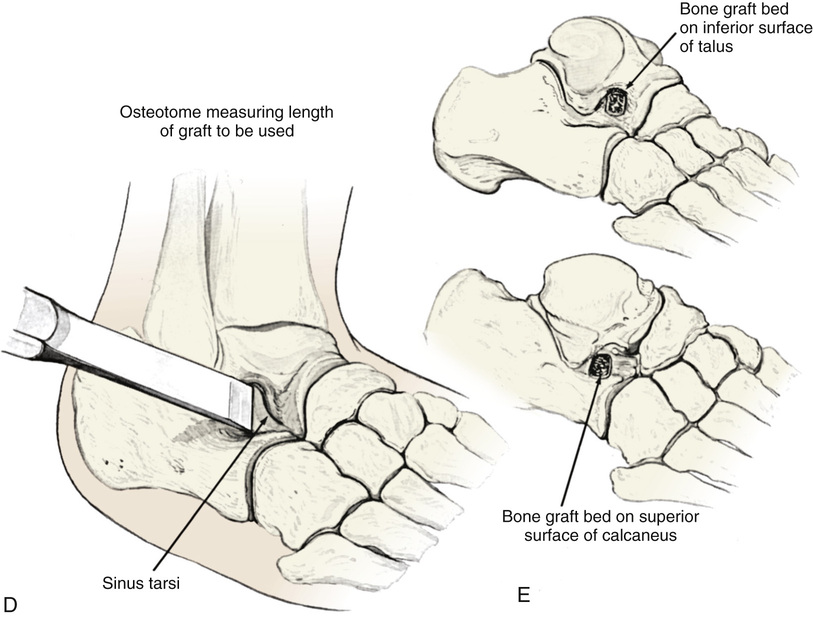
D, Next, the foot is manipulated into equinus position and inversion while rotating the calcaneus into its normal position beneath the talus and correcting the valgus deformity. Broad straight osteotomes of various size ( to
to  inches or more) are inserted into the sinus tarsi to block the subtalar joint and determine the length and optimal position of the bone graft and the stability that it will provide. The long axis of the graft should be parallel to the long axis of the leg when the ankle is dorsiflexed into neutral position.
inches or more) are inserted into the sinus tarsi to block the subtalar joint and determine the length and optimal position of the bone graft and the stability that it will provide. The long axis of the graft should be parallel to the long axis of the leg when the ankle is dorsiflexed into neutral position.
E, The optimal site of the bone graft bed is marked with a broad osteotome. A thin layer of cortical bone ( to
to  inch) is removed with a dental osteotome from the inferior surface of the talus (the roof of the sinus tarsi) and the superior surface of the calcaneus (the floor of the sinus tarsi) at the site marked for the bone graft. It is best to preserve the most lateral cortical margin of the graft bed to support the bone block and prevent it from sinking into soft cancellous bone.
inch) is removed with a dental osteotome from the inferior surface of the talus (the roof of the sinus tarsi) and the superior surface of the calcaneus (the floor of the sinus tarsi) at the site marked for the bone graft. It is best to preserve the most lateral cortical margin of the graft bed to support the bone block and prevent it from sinking into soft cancellous bone.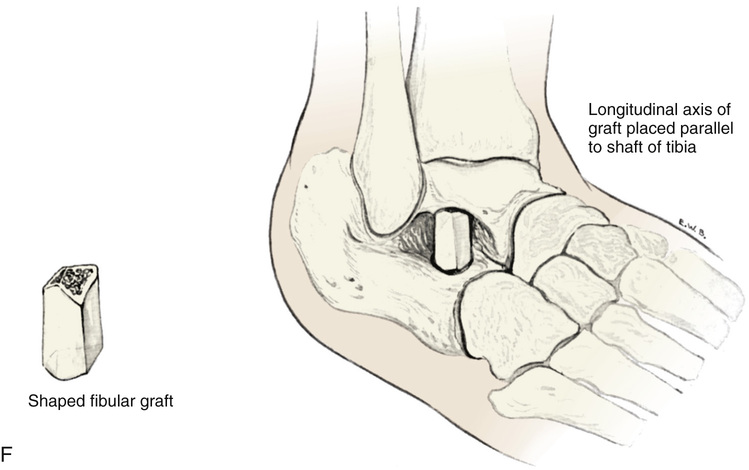
F, A bone graft of appropriate size can be taken from the fibula or iliac crest. The corners of the base of the graft are removed with a rongeur so that the graft is trapezoidal in shape and can be countersunk into cancellous bone to prevent lateral displacement after surgery.
The bone graft is placed in the prepared graft bed in the sinus tarsi by holding the foot in varus position. An impactor may be used to fix the cortices of the graft in place. The longitudinal axis of the graft should be parallel to the shaft of the tibia with the ankle in neutral position.
With the foot held in the desired position, the distal soft tissue pedicle of fibrofatty tissue of the sinus tarsi, the calcaneal periosteum, and the tendinous origin of the short toe extensors are sutured to the reflected periosteum from the talus. The subcutaneous tissue and skin are closed with interrupted sutures, and a below-knee cast is applied.
Postoperative Care
The cast is removed 8 to 10 weeks after surgery. If radiographs show solid healing of the graft, gradual weight bearing is allowed with the protection of crutches. Active and passive exercises are performed to strengthen the muscles and increase range of motion of the ankle and knee.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


