Anteromedial Approach to a Developmentally Dislocated Hip
Surgical Anatomy
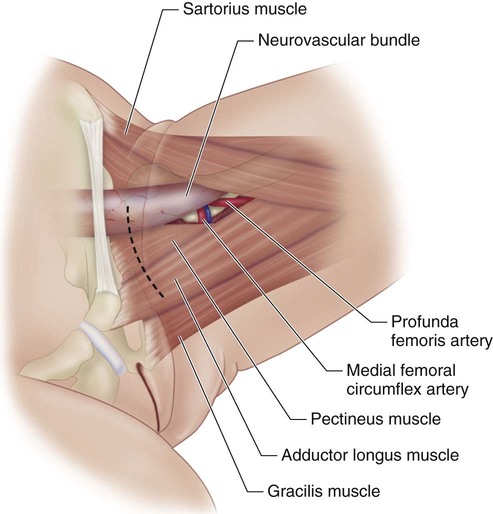
 The key anatomic relationships to understand in the anteromedial approach are the relationship of the neurovascular bundle to the pectineus; the location of the medial femoral circumflex vessels; the relationship of the anterior branch of the obturator nerve to the adductor longus and brevis; the relationship of the lesser trochanter and the iliopsoas tendon to the neurovascular bundle and the pectineus; and finally the relationship of the anteromedial hip joint capsule to the overlying structures.
The key anatomic relationships to understand in the anteromedial approach are the relationship of the neurovascular bundle to the pectineus; the location of the medial femoral circumflex vessels; the relationship of the anterior branch of the obturator nerve to the adductor longus and brevis; the relationship of the lesser trochanter and the iliopsoas tendon to the neurovascular bundle and the pectineus; and finally the relationship of the anteromedial hip joint capsule to the overlying structures.
 Figure 1 shows the relevant surgical anatomy for this procedure.
Figure 1 shows the relevant surgical anatomy for this procedure.
Portals/Exposures
 The groin crease is identified as well as the superior and inferior borders of the adductor longus in the groin crease. The incision should extend from just inferior to the femoral neurovascular bundle in the groin crease to the inferior border of the adductor longus. The skin and subcutaneous tissues are incised sharply down to the deep fascia. This fascia is incised longitudinally with a #15 blade along the adductor longus in the direction of the muscle fibers for about 2–3 cm.
The groin crease is identified as well as the superior and inferior borders of the adductor longus in the groin crease. The incision should extend from just inferior to the femoral neurovascular bundle in the groin crease to the inferior border of the adductor longus. The skin and subcutaneous tissues are incised sharply down to the deep fascia. This fascia is incised longitudinally with a #15 blade along the adductor longus in the direction of the muscle fibers for about 2–3 cm.
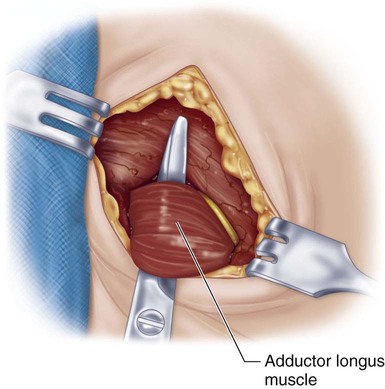
 The adductor longus is isolated using dissecting scissors (Fig. 2). The anterior branch of the obturator nerve is seen on the anterior surface of the adductor brevis muscle below the adductor longus; this nerve should be protected. The adductor longus muscle is sectioned close to its insertion with bipolar cautery. The anterior branch of the obturator nerve is once again identified as it crosses the adductor brevis muscle and protected.
The adductor longus is isolated using dissecting scissors (Fig. 2). The anterior branch of the obturator nerve is seen on the anterior surface of the adductor brevis muscle below the adductor longus; this nerve should be protected. The adductor longus muscle is sectioned close to its insertion with bipolar cautery. The anterior branch of the obturator nerve is once again identified as it crosses the adductor brevis muscle and protected.
Related posts:
![]() 41: Operative Treatment of Tillaux Fractures of the Ankle
41: Operative Treatment of Tillaux Fractures of the Ankle
![]() 15: Repair of Proximal Hamstring Avulsion
15: Repair of Proximal Hamstring Avulsion
![]() 28: Femur Fracture: Closed Reduction and Spica Cast
28: Femur Fracture: Closed Reduction and Spica Cast
![]() 18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
![]() 47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


20: Anteromedial Approach to a Developmentally Dislocated Hip








